

A common problem in distance runners and change-of-direction sports like football, soccer, and hockey, proximal hamstring tendinopathy is a pain in the butt (literally)! Characterized by deep, localized pain over the ischial tuberosity (the large, bony protuberances/bumps on your bottom), this often gets worse with running, lunging, squatting and sitting (1). Often challenging to initially recognize, and located in an area with lots of potential pain generators, proximal hamstring tendinopathy can truly be a bear to manage and resolve. Luckily, there are lots of conservative management options, with therapeutic exercise prescription being a top choice. If it sounds like we’re hitting the mark for what you’re experiencing with a high hamstring injury, or you’re just interested to learn about this common injury, you’ve come to the right place. Read on to learn more.
Setting the Stage
A muscle group is commonly known to the public, and often better recognized by the stereotypical, sports medicine distress call of “I just pulled a hammy!”, the hamstring musculature gets a ton of recognition. In an NFL team data publication tracking injuries from 1998 to 2007, hamstring strains were found to be the most common muscle strain and the second most common injury (2). A similar publication with injury data from 51 professional soccer teams reported hamstring strains as the most common injury, representing 12% of all injuries overall (3). With lengthy rehab and recovery times, lasting anywhere between 23 days (4) and 50 weeks (5), extensive amounts of money are often lost to missed playing time in the professional realm. Outside of high-level sports, hamstring strains are especially common in the general public as well, sometimes presenting on both sides at once (1). But how does this even happen in the first place? Let’s break this down a bit further, jumping into some of the relevant anatomy and common mechanisms of injury.
Dealing With A Hamstring Injury? We’ve Got You Covered!

Hamstring injuries are one of the most common soft tissue injuries in sports. They are especially challenging and frustrating due to the high recurrence rate. This is largely because people don’t appropriately rehab their injuries. It’s time to change the narrative and be proactive with taking care of your hamstrings! This program will expose your hamstrings in a safe and effective manner to prepare you for high-level activities! Learn more HERE!
Anatomy and Mechanisms of Injury
If you didn’t know, your hamstrings are actually a complex of 3 different muscles: the biceps femoris (comprised of both a short head and long head), semitendinosus and semimembranosus. All of the hamstring musculature, with the exception of the short head of the biceps femoris, originate from the ischial tuberosity (6), often referred to as your “sit bone.” The majority of this musculature spans across the hip and knee joints, allowing it to provide both hip extension and knee flexion.

A nice illustration of the hamstring complex: semitendinosus and semimembranosus on the left, and your biceps femoris on the right. The semitendinosus and biceps actually share the same origin, while semimembranosus inserts more laterally (image from Arner et al, 2019).
Hamstring injuries can occur anywhere along the length of the musculature, but are typically separated into proximal (up towards your sit bone), muscle belly (towards the middle), and distal injuries (where the muscle inserts below the knee joint) (6). The anatomy of this muscle is what allows it to provide so much function for us, however, it also predisposes the hamstrings to injury. The greatest strain on this musculature occurs during the end of the swing phase when the hamstrings eccentrically contract at their maximal elongation before heel strike (6,7), often during high speed running. This mechanism of injury tends to occur most commonly in the free tendon of the semimembranosus (8). But to be fair, there is also a camp of thought that believes the hamstrings are also at risk for injury during the early stance phase of sprinting as well (7,9). Both positions likely contribute to scenarios where the hamstrings are most at risk.
There are numerous proposed risk factors for hamstring injury including decreased flexibility, strength deficits, muscle fatigue, poor core stability, lack of proper warm-up, poor lumbar posture, and prior hamstring injury (7). This all being said, a prior hamstring injury has been shown to increase the risk of recurrence two to six times (10-12). It’s thought that reparative scar tissue serves as a stress riser lowering the threshold adjacent to normal tissue (6).
So now that we’ve set the stage surrounding hamstring injuries, we’re going to focus specifically on proximal hamstring tendinopathy. Appreciate that the proximal hamstring can avulse (pull off of its attachment) or tear, and these can change medical management quite a bit. Generally, injuries of this caliber will present with extensive discoloration/bruising and/or a very specific, high-force mechanism of injury. A detailed medical examination, with imaging when warranted, can help get you on the right management pathway.
LISTEN: HAMSTRING INJURIES WITH DR. SHANE NHO

What is a tendinopathy?
Tendinopathy occurs in loaded tendons resulting in decreased exercise tolerance and a reduction in function. Literal changes occur in the tendon structure, resulting in a tendon that is less capable of sustaining repeated tensile load (13). In short — the tendon becomes painful, and it sucks. Proximal hamstring tendinopathy is considered to be insertional tendinopathy, with the thought that compression of the tendon at its attachment during hip flexion is a major contributor to its development (1).
A concept often discussed in unison with tendinopathy is tissue capacity. In essence, a tissue is at full capacity when an individual is able to perform functional movements at the volume and frequency required without exacerbating symptoms or causing tissue injury (14). When a tissue experiences a loading event that exceeds its tissue capacity, a musculotendinous or ligament injury occurs (14). The names of actual injuries may vary including musculoskeletal diagnoses like sprains, strains, tendinopathies, or ruptures.
In tendinopathy, the tissue response is usually more gradual. Considering the unique anatomy of the hamstring and mechanisms of injuries we’ve already discussed, it’s common for proximal hamstring tendinopathies to develop secondary to increasing volume too quickly, suddenly introducing sprinting, lunging, hurdles, or hills (15,16) — all of these require the hamstring to contract or lengthen while in hip flexion, putting provocative tensile and compressive load at the tendon insertion (17,18). In sedentary individuals, compressive loading just from sitting can be the main load-inciting factor (19). Imagine the differences in tissue capacity between a wide receiver getting injured on his first day of training camp and a deconditioned office worker putting in extra hours at their desk; tissue capacities will vary significantly, as will their respective mechanisms of injury. However, the themes discussed here remain the same. It largely comes down to tissue capacity.
Want to learn more about tendinopathies? Read this article!
READ: TENDINITIS VERSUS TENDINOSIS

What can I do to treat this?
The key to management of all tendinopathies includes load modification and progressive loading, performed within a pain-monitoring framework, to initially reduce pain and later restore function (1). These are the bread and butter of a well-trained sports physical therapist, athletic trainer, strength and conditioning coach, or chiropractor; any of these rehabilitative personnel should be able to help get you started. But regardless of whether you seek one of these professions, let’s dive into both of these topics deeper. Learn more about the key to progressive overload!
Load Modification
Load modification initially includes identification of the tendinopathy, and appreciation that its load capacity has been exceeded. A discussion should be held with the patient (or can take place personally through a training journal) over recent training trends detailing intensity, duration, and overall load. Was there a spike in one of these variables that precipitated the tendinopathy? I’d be willing to bet so. Now thankfully, It doesn’t mean we have to back off training to the point the patient loses their level of fitness, rather, the patient will need to be conscious of their pain levels and follow stable pain guidelines.
In general, someone with tendinopathy can continue their sport or hobby, so long as their pain levels remain at or below a “3” on a scale of “1 to 10.”
Often enough, athletes will find they can still continue some steady-state running (1) but will find they struggle with hills, starts, and hurdles. In other words, load management of proximal hamstring tendinopathy often involves limiting abusive compressive (hip flexion) and energy storage loads until pain irritability settles to a stable level (1). For someone more sedentary trying to limit compressive loads that accompany sitting, it’s not a bad idea to try a standing desk or using a specially shaped cushion that re-distributes compression off of the ischial tuberosities and onto the posterior thigh/muscles (1). Read more on working desk posture tips HERE!
Quick Tips For Rehabbing A High Hamstring Injury
Progressive Loading
Increasing tendon capacity through rehabilitation with gradual tendon loading, more often than not, reduces pain and improves function eventually allowing the patient to return to their hobby or sport (14). Previously, the medical model traditionally would recommend complete rest — we now know that this is far from best practice, despite many clinicians still recommending this to patients today. Presently, there is no clear rehabilitative guidance in the literature regarding proximal hamstring tendinopathy. However, general themes exist (1) that we’re going to outline in stages next. A patient need not follow these in a textbook fashion, but there are general themes that should probably be honored. Just like dietitians are generally reluctant to label specific foods as “magic,” a good physical therapist generally should feel the same about specific exercises. That being said, there are a few niche exercises that are likely worth programming into your rehabilitation.
Exercises for Proximal Hamstring Tendinopathy
Please keep in mind, that there are many different routes to the successful rehabilitation of proximal hamstring tendinopathy. Rehabilitative specialists often “live in the gray.” There are so many right answers, and so little few wrong, that we all program with slightly different tastes. Generally, after 48 hours of rest following the initial injury, exercise programming can begin. That being said, these suggestions below serve as guidelines — not gospel. Listen to your musculoskeletal healthcare provider and trust the process.

The Prehab membership is the anti-barrier solution to keeping your body healthy. Access state-of-the-art physical therapy, fitness programs, and workouts online in the comforts of your own home or gym! Taking control of your health with exercise & education from the palm of your hand has never been easier. Get access to 50+ programs, 100+ unique workouts, and 3000+ exercises to build your own workout routines. Trial it for free, and learn how to get out of pain, avoid injury, and optimize your health with [P]rehab!
Stage 1: Isometric Hamstring Load
An isometric exercise is a form of muscle contraction where you build tension in the muscle, but the actual fibers don’t change length. It is generally celebrated in the rehabilitative health care community for its appropriateness in post-surgical neuromuscular re-education and the generalized pain inhibitory response it provides (20). If you’re looking for an elevator pitch for isometric exercises: it allows us to gently and effectively load the muscle-tendon unit and generally reduce pain in those with irritable symptoms. Dosage should be based on symptom severity and irritability, but researchers have generally advocated for 5 sets of 45-second holds of moderate-resistance isometric exercise performed at 70% maximal voluntary isometric contraction (21). If you’re unable to perform to these recommendations, decrease the intensity of your contraction to meet our pain guidelines of remaining at, or below a “3” out of “10.”
As I’ve said about 10 times in 10 different ways already — there are many ways to program to these standards. However, here are some of my personal favorites published by Goom, Malliaras, Reiman and Purdam (1).
Single-Leg Bridge Hold
Single-Leg Bridge Hold (Long-Lever)
Noraxon / Biodex Isometric Hamstring Curl
Stage 2: Isotonic Hamstring Load with Minimal Hip Flexion
So you’re no longer experiencing pain with your isometric programming. That means you’ve generally graduated from hamstring isometrics! That doesn’t mean you can’t continue to utilize them in your programming, but as your tissue capacity increases, so does the level of your programming. We’ll now shift our focus to isotonic exercise. Isotonic contractions occur when a muscle contracts and fibers actually change length while lifting an external load. Breaking this term down even further, an isotonic exercise includes both concentric and eccentric contractions. In a concentric contraction, muscle fibers shorten. In an eccentric contraction, muscle fibers lengthen. Regardless of contraction type, our aim in this stage is to restore hamstring strength, bulk, and capacity in a functional range of motion (1).
Previously, eccentric exercise has been championed as the contraction type of choice in the treatment of tendinopathy. It certainly holds value, as you’ll see with some of the specific programmings up next, but heavy slow resistance training is generally becoming the exercise treatment of choice in the tendinopathy realm. The magnitude of load determines the effect on tendon and muscle adaptation, rather than contraction type (22). That being said, it’s recommended in this stage to focus on slow, fatiguing, resisted isotonic exercise with a weight selected that fatigues by 15 repetitions. Later, this should be progressed to 8 repetitions, which will obviously allow for an increase in weight. 3 to 4 sets should be performed every other day (23).
The angle at your hip during isotonic will be allowed a bit more flexion (compared to exercises in stage 1 where the hip was generally kept to 0 degrees), introducing a bit more compression at the ischial tuberosity. Although the trend of your programming in this stage is moving away from isometrics, I personally like to begin introducing manual spectrum isometrics here as well (if tolerated). This all being said, see a few examples below that are appropriate for this stage. Remember, throughout all of this, we’re keeping our pain management guidelines in check (no more than a “3” out of “10” on a numeric pain scale). Listed below are 3 different ideas to incorporate into your programming of this stage.
Nordic Hamstring Curls
Single Leg Supine Physioball Eccentrics
Manual Spectrum Hamstring Isometrics
Stage 3: Isotonic Hamstring Load with Hip Flexion
By this point, you’re likely starting to feel pretty good again. However, we haven’t really focused on the positioning you likely found yourself injured in the first place: those deep, end ranges of hip flexion. The goal in this stage remains the same as stage 2: continue improving hamstring strength and encouraging hypertrophy, except now we’re venturing into deeper ranges of hip flexion (1). Our dosing stays the same as well, occurring every other day (1). Our pain guidelines additionally stay the same here as well, however, with a significantly higher degree of awareness/monitoring. Many of these exercises may be, to some degree, provocative. Stay the course, follow the rules, and don’t stress should they be mildly irritating. As we’ve established, no higher than a “3.”
Now, I’m admittedly a bit biased, but in 2012 a newer concept in hamstring injury rehabilitation/prevention emerged and was published by two therapists, Tim Tyler and Brandon Schmitt. At the time, these two were my mentors and continue to serve as such today. These guys wrote a great publication on the value of performing hamstring eccentrics in the lengthened state (7). In most physical therapy programming, hamstring exercises are only performed between 0 and 90 degrees of hip flexion. These researchers argue we should pursue even deeper angles in our programming.
Now, we’ve discussed that eccentrics serve some value, but heavy and slow resistance training is likely most paramount in the fight to improve load capacity. This still ultimately holds true in loading for tendinopathy rehabilitation. However, I personally believe hamstring eccentrics in the lengthened state to be a missing piece in the majority of hamstring rehabilitation performed today. What better way to improve load capacity — with an added element of specificity — than training in the position our hamstrings are most susceptible to? Training in the lengthened state may help shift the curve to acquire the necessary eccentric strength at the end range of motion to avoid susceptibility to further injury (7). In addition, it should likely always be included in the late-stages of a complete hamstring rehabilitation. We’re going to discuss it in length together here below, but I encourage you to read the original article here.
Hamstring Eccentrics in the Lengthened State (Biodex, Cable Column, Manual)
Now the best way to perform this exercise is with a Biodex — a specialized piece of rehab equipment found typically only in physical therapy clinics. With a specialized attachment, the hip is raised into deep angles of flexion. In the photo below, our athlete is pictured at the end of a repetition. The machine is slowly raising up her foot towards the ceiling while she actively tries to resist. It’s a damn hard exercise!
a. Biodex

An athlete performing lengthened state eccentric training on the Biodex (7).
Now chances are, you likely don’t have access to this piece of equipment. Although it’s the gold standard, there are two other options. This can be performed on a cable column or can be performed manually with the help of a therapist or friend. Both options are listed below.
b. Cable Column
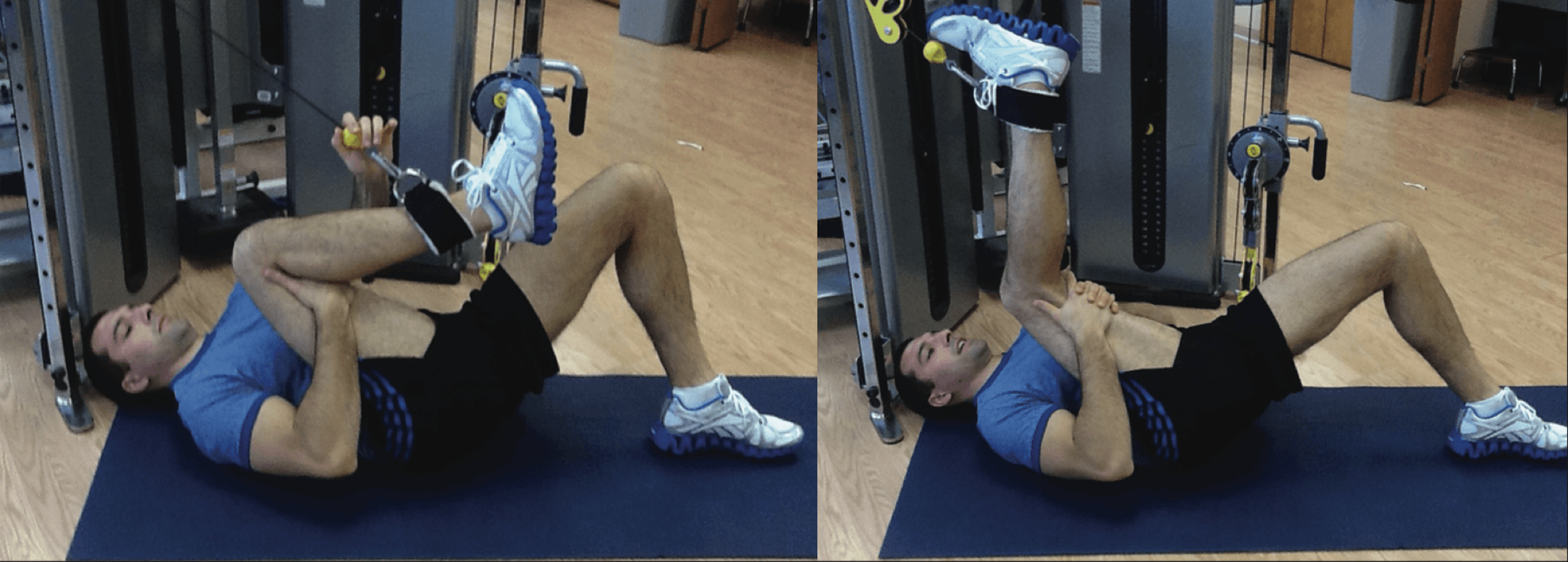
(Left) Laying supine on the ground, with your hip into end-ranges of deep hip flexion, assist your knee into full flexion by unweighting the cable. (Right) Afterwards, remove your hand that provided the extra assist, and slowly resist the weight, extending your knee into full extension (7).
Hamstring Eccentrics Manual Resistance
Romanian Deadlifts
- HOW: Position a barbell in front of you on the ground over the middle of your feet. Find your “power stance” with your feet roughly shoulder width apart. Hinge forward at the waist, grip the bar slightly wider than your knees, keep some tension in your legs with your knees slightly bent, squeeze your shoulder blades back, push into the ground with your feet and lift the bar up to your waist, always keeping a small bend in your knees.
- FEEL: You should feel your lower body muscles working as well as your glutes and back.
- COMPENSATION: Keep your back flat, don’t arch it. Control the weight going up and down.
Stage 4: Energy Storage Loading
The fourth and final stage of proximal hamstring tendinopathy programming will focus in heavily on lower-limb energy storage/impact loading (1). Naturally, only athletes need to complete this stage in full. This phase should be started once phase 3 has been fully established as pain-free. Out of all the 4 stages, this one certainly has the most opportunity for creativity and interpretation. It’s where a great sports physical therapist will shine, selecting programming that replicates the demands of sport (running, sprinting, jumping, and lifting). We won’t dive into the specifics here, but this phase should involve lateral, rotational, and cutting movements to graduate loads in multiple planes of movement (1). Care should continue to be taken with adding in hill and speed training sessions, as these can still be a bit provocative.
Once you can tolerate all the loading requirements of your sport, a graded return to sport can be introduced, working back into a full return to play. To be fair, there are some specialized tests that can be performed to ensure an athlete is truly ready for return to play (limb symmetry index), but that’s another article for another day.
Closing Thoughts
- To close, the proximal insertion of the hamstrings are especially susceptible to tendinopathy due to their anatomy and a unique mechanism of injury often seen in high-level sport.
- Tendinopathies respond best to load, but the load should be prescribed in a graded and thoughtful manner.
- Activity modification should be taking place while completing a full hamstring rehabilitation program.
- Placing yourself, or an athlete, on an extended period of rest will do more harm than good. This was a common recommendation in the past; the field has moved on from this.
- There are many right answers, and so few wrong, in the rehabilitative programming for proximal hamstring tendinopathy. Begin with isometrics and progress to isotonics. Begin with no hip flexion, progress to small angles of hip flexion, and finish with large angles of hip flexion. Gradually introduce sport-specific movements, being careful with hills and speed work.
- There are no “magic exercises,” however, nordic hamstring curls and hamstring eccentrics in the lengthened state are two valuable pieces in this puzzle.
Take Control of Your High Hamstring Injury

Hamstring injuries can be straightforward or can disguise themselves as false sciatic pain or piriformis syndrome. In either case, the solution becomes the same: early movement that protects the area while creating enough of a stimulus to become stronger!
References
About The Author
Christopher Lefever, PT, DPT, SCS, CSCS, USAW
[P]Rehab Writer & Content Creator
 Originally from Reading, Pennsylvania, Chris graduated with his bachelor’s degree in exercise science and a doctorate of physical therapy from Slippery Rock University. He afterwards completed a sports physical therapy residency at the Memorial Hermann IRONMAN Sports Medicine Institute. He later completed a division 1 sports physical therapy fellowship at Duke University where he worked closely with Duke football, basketball and lacrosse. He returned to Houston afterwards with Memorial Hermann to help develop an emerging division 1 sports physical therapy fellowship. Present day, he practices with the sports medicine team at the United States Olympic and Paralympic Committee in Colorado Springs, CO. Chris is board certified sports clinical specialist (SCS), certified strength and conditioning specialist (CSCS) and certified in dry needling. He has a particular interest in post-operative rehabilitation of the athletic knee, shoulder, hip and elbow.
Originally from Reading, Pennsylvania, Chris graduated with his bachelor’s degree in exercise science and a doctorate of physical therapy from Slippery Rock University. He afterwards completed a sports physical therapy residency at the Memorial Hermann IRONMAN Sports Medicine Institute. He later completed a division 1 sports physical therapy fellowship at Duke University where he worked closely with Duke football, basketball and lacrosse. He returned to Houston afterwards with Memorial Hermann to help develop an emerging division 1 sports physical therapy fellowship. Present day, he practices with the sports medicine team at the United States Olympic and Paralympic Committee in Colorado Springs, CO. Chris is board certified sports clinical specialist (SCS), certified strength and conditioning specialist (CSCS) and certified in dry needling. He has a particular interest in post-operative rehabilitation of the athletic knee, shoulder, hip and elbow.
Disclaimer – The content here is designed for information & education purposes only and is not intended for medical advice.
About the author : Chris Lefever
Related posts



Latest Blogs

Get Proactive with Prehab
- ✔ Zero wait times, no hidden fees, no barriers to entry!
- ✔ Get out of pain, get stronger, and improve your mobility
- ✔ Access to easy-to-digest physical therapy education videos & resources to learn about your body in the palm of your hand
- ✔ Guidance from trusted Doctors of Physical Therapy








