






Bone Stress Injuries (BSI) are not uncommon in avid runners, track and field athletes, and endurance athletes. As common as they may be, they are still very difficult to deal with, hard to identify for the average person, and unfortunately can turn into full-blown bone stress fractures before being correctly identified and treated. In this article, we will discuss exactly what bone stress injuries and bone stress fractures are, what the risk factors are, and prehab strategies to get back to running after a bone stress fracture.
What Is A Bone Stress Injury (BSI) & A Bone Stress Fracture?
Bone stress injuries (BSI) in runners result from the failure of the skeletal bones to withstand repetitive, submaximal forces. BSI can range in severity as well as location, with early injuries showing varying degrees of bone edema on an x-ray versus more advanced stress fractures showing evidence of a fracture line (1). According to an article by Pegrum et al. 2012, “stress fractures occur as a result of overuse injuries to bone, either secondary to bone fatigue or bone insufficiency. Fatigue stress fractures occur when the normal bone is unable to keep up with repair when repeatedly damaged or stressed. Insufficiency stress fractures, however, occur in the bone that is under normal strain but structurally abnormal because of metabolic bone disease or osteoporosis.”
It is beneficial to have a great understanding of tissue healing in regards to prognosis and treatment. Bones for example usually have good healing properties due to their abundant blood supply, which is needed for quality tissue healing. Check out this graphic below on tissue healing times based on different types of tissue in the body! Thank you to Dr. Caleb Burgess for this excellent graphic!
Healing Times Based on Tissue Type
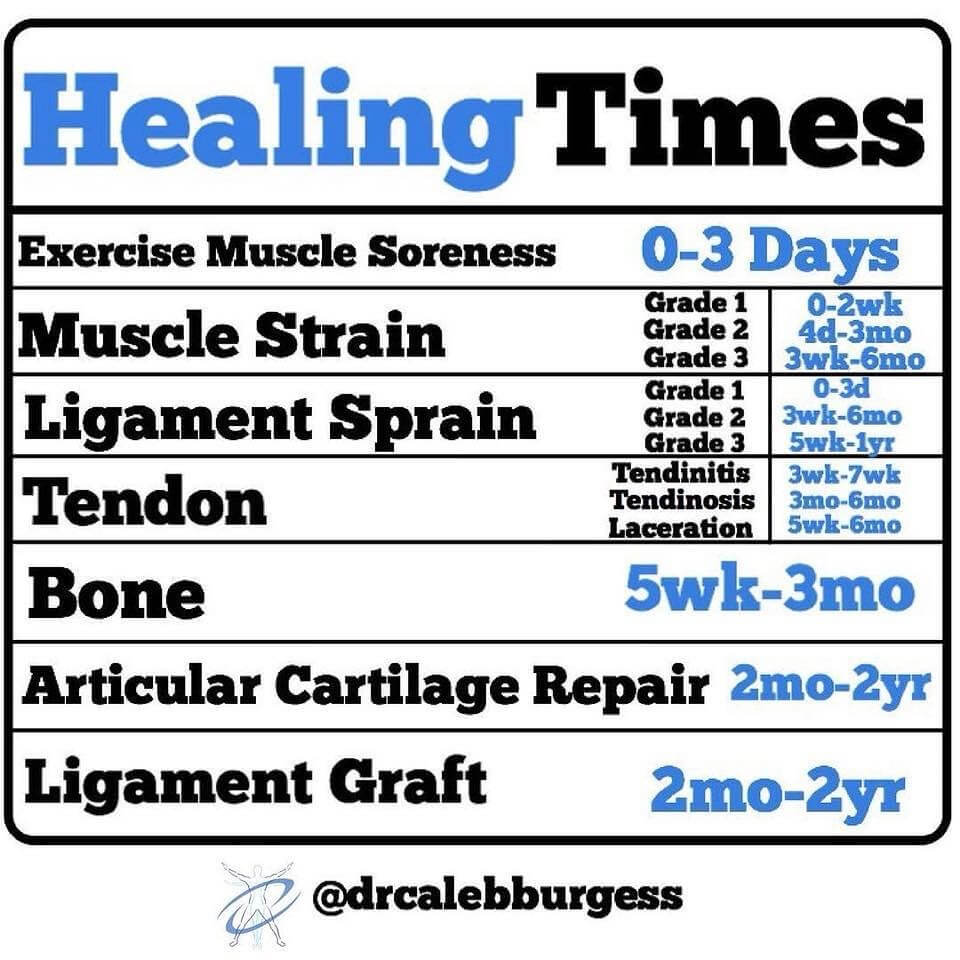
From Dr. Caleb Burgess
You will notice in this graphic that bone healing can span from 5 weeks – 3 months on average. There are many factors that play a role in tissue healing for each individual besides the property of the tissue itself, including healing environment, lifestyle, health, and much more.
What Are The Incidence Rates & Risk Factors?
According to an article by Tenforde et al. 2016, “studies suggest the annual incidence of BSI may be greater than 20% in runners and that BSI is a common cause of injury in track and field athletes.” Another group has suggested that up to 20% of sports medicine consultations every year are for bone stress fracture injuries (2).
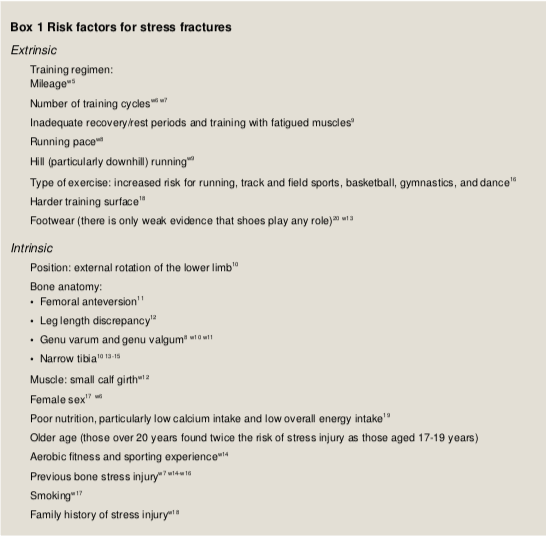
Research into bone stress injuries and bone stress fractures in regards to running and other sports have identified two groups of risk factors that contribute to these types of injuries. Intrinsic risk factors are those that are inherent to you including your gender, genes, medications you take, nutrition, and your body type and build. With intrinsic risk factors, some of them are non-modifable risk factors meaning you have little to no control over being able to influence them. For runners specifically, intrinsic risk factors are more signifciant to consider for females compared to males as being a female is a risk factor for bone stress fractures.
Extrinsic risk factors, on the other hand, are those that are shaped by the environment you immerse yourself in. In regards to running, this includes your running mileage, your training schedule, the route(s) you take, the surface you run on, the shoes you wear, the pace you run at, and more. Below is an extended list of both risk factor groups
Risk Factors For Stress Factors
Relative Energy Deficiency in Sport (RED-S)
If you’re a runner you’ve likely heard the term – the female athlete triad. However, this term has been replaced by RED-S. The female athlete triad referred to the presence of low bone mineral density or disordered eating, low body mass index (BMI), and menstrual irregularity or prolonged absence of menses. However, RED-S was adopted to include males and emphasize that it’s often not associated with an eating disorder and shift the focus to either insufficient caloric intake and/or excessive energy expenditure. The consequences of RED-S can lead to negative physiological changes.
In females especially, being energy-deficient with low BMD/BMI increases the athlete’s risk of bone stress injuries and bone stress fractures (2). This is why it is extremely important to do your due diligence as a healthcare professional, a parent, or a coach when working and dealing with female runners who are experiencing lower limb or even low back/pelvic pain. It often takes a team effort to help female athletes when dealing with these types of injuries. It is even more important to consider prehab strategies with female athletes who have had a bone stress injury or bone stress fracture in the past. You can learn more about RED-S by clicking here.
Want To Return To Running After An Overuse Injury?

A lot of people think that you can just grab a pair of shoes and start running, which can be true. However, failure to prepare may set you up for failure. “You don’t run to get fit, you have to be fit to run.” Without proper training, education, and an understanding of healthy running hygiene habits, issues may arise that can keep you from running. The Running [P]Rehab Program will teach you the best cross-training routine for runners and education to help you maintain optimal running health. Learn more HERE!
What Are The Common Locations?
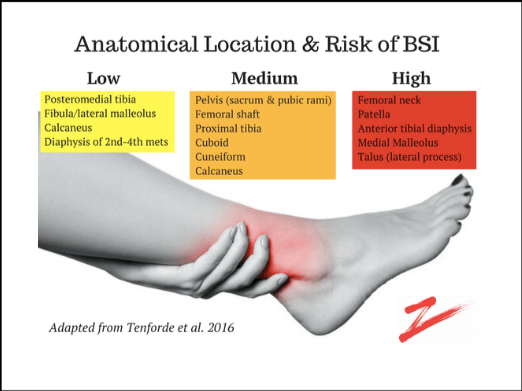
Common sites for bone stress injuries and bone stress fractures are primarily in the lower body. The common locations include the femur, tibia, fibula, and bones in the foot including the metatarsals, tarsals, and calcaneus (1). Based on the understanding of the biological healing process, knowledge of blood supply to the bone in different areas of the body, and the direction of loading on the bone, these locations have been separated into low, medium, and high risk of fracture non-union – meaning the chance of the bone failing to heal unless intervention, such as surgery, is performed.
Locations And Risk Quantities of Bone Stress Fractures
Diagnosing Bone Stress Injuries & Stress Fractures
Ultimately the gold standard for identifying and diagnosing bone stress injuries and bone stress fractures is using Magnetic Resonance Imaging (MRI). MRIs are the most sensitive and specific imaging modality compared to normal radiographic images (x-rays) as these images can appear normal for the first few months despite clinical signs and symptoms of a bone stress injury. It typically takes a bone stress injury to fully progress to a bone stress fracture to see changes on an X-ray. With early imaging via an MRI, a bone stress injury can be detected, which can lead to appropriate intervention in efforts to avoid a full-blown bone stress fracture and delayed recovery time (2). This is one of the few instances that we support early imaging – if a bone stress injury or bone stress fracture is suspected – as this can truly change and dictate the next course of action.
Imaging recommendations should be based on a thorough evaluation of the individual’s demographics, medical history, training history, mechanism of injury, and clinical signs and symptoms. In general, bone stress injuries are initiated by a bone stress reaction and typically present with focal tenderness to palpation at the bone site. Pain is experienced at the bone site with training and physical activity. Progressive bone stress injuries and bone stress fractures will present with pain after activity including pain at rest and pain with simple day-to-day activities (2).
Learn The Most Important Exercises For Runners
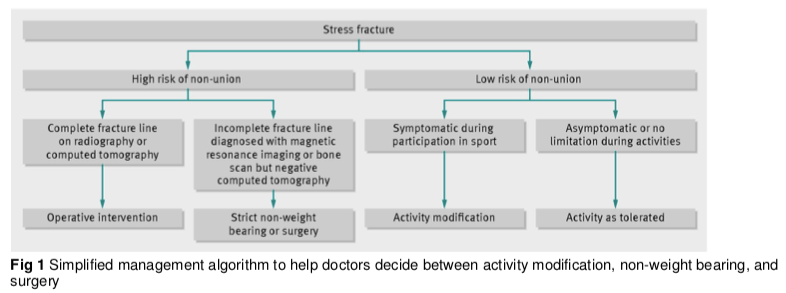
Bone Stress Fracture Management
Below is a simplified algorithm by Pegrum et al. 2012’s group to understand the steps taken following the identification of a bone stress fracture.
[P]Rehab Strategies For BSI & Bone Stress Fractures
There are multiple things to take into consideration in efforts to avoid bone stress injuries and bone stress fractures. It all comes back to analyzing the risk factors, ultimately prehab is based on a needs analysis and the specificity of the activity. If we consider non-modifiable risk factors such as gender, age, unfavorable boney anatomy, and family history of BSI – simply having awareness that you’re more prone to these types of injuries will help you make smarter informed decisions about managing modifiable risk factors. These include…
- Physical Fitness Level (get fit to run, don’t run to get fit)
- Training Volume (smart program periodization, cross-training, mileage, intensity, recovery)
- Nutrition (calcium and vitamin D intake, caffeine intake, smoking, energy availability)
- Stress (rest, sleep, physical and psychological life stressors)
- Targeting Strengthening (if you have a history of foot BSI – be sure to include more calf and foot intrinsic strengthening exercises)
We feel confident in saying >90% of the running injuries we see in the clinic are due to training errors. The more educated you are about the physical activity you want to perform and the musculoskeletal risks associated with it, the more likely you’ll be able to make smart prehab decisions for your body.
READ: RUNNER’S KNEE CAUSES AND TREATMENT

Return to Running After A Bone Stress Fracture
So what if you’re already dealing with a bone stress injury or a bone stress fracture? How do you get back to running? Below we will identify what we believe are the appropriate steps to manage these types of injuries.
- Accurate Diagnosis – consult with healthcare professionals that have experience with treating runners. Work with someone like a physical therapist and an orthopedist to assess you and ensure early and accurate identification of a bone stress injury or bone stress fracture as better results are associated with earlier identification of these types of injuries.
- Activity Modification – The sooner these types of injuries are accurately identified, the sooner you can modify your activity and work on modifiable risk factors to protect the bone and let it heal. This may mean a time period of non-weightbearing or no high-impact physical activity. This will depend on the injury site and whether it is a low or high risk non-union site. However, this doesn’t mean complete rest! Find a physical therapist that will prescribe appropriate exercises to stay as strong and fit as you can to avoid deconditioning.
- Graded Exposure – For more common low-risk bone stress injury and bone stress fracture sites like the posteriormedial tibial shaft, once you no longer have pain at rest or with daily activities you can start to gradually re-introduce physical activity and bone loading. This is in-conjuction with continuing to address modifiable risk factors and truly listening to your body while keeping track of your physical activity. One of our favorite phrases is you cannot manage what you don’t measure, keeping track of your steps, time on your feet, your workouts, and your runs early on can help you gradually increase load on the bone without doing too much too soon. Without measuring important variables, it is hard to safely progress loading and more importantly reflect back on what you did that may have caused a setback in your rehab and recovery.
- Seek Professional Help – If you’re dealing with what you believe to be a bone stress injury or bone stress fracture and it hasn’t improved in months, seek professional help. As stated earlier – these types of injuries, especially in high-risk fracture non-union locations, should not be taken lightly in efforts to avoid delayed recovery and/or surgical intervention.

The Prehab membership is the anti-barrier solution to keeping your body healthy. Access state-of-the-art physical therapy, fitness programs, and workouts online in the comforts of your own home or gym! Taking control of your health with exercise & education from the palm of your hand has never been easier. Get access to 50+ programs, 100+ unique workouts, and 3000+ exercises to build your own workout routines. Trial it for free, and learn how to get out of pain, avoid injury, and optimize your health with [P]rehab!
Axial Loading Exercises After A Bone Stress Fracture
When appropriate/tolerated well with no pain during/after activity and minimal to no soreness after 24-48 hours, progressive axial loading exercises need to be performed. These types of exercises are necessary to optimally load the bone so that it can tolerate repetitive, submaximal forces that occur with high-impact activities like running. Below are a few examples of different exercises we like to incorporate within a cross-training program for runners.
Marching
Sample [P]rehab Running Program Exercise
Simple movement acquisition that mimics running is essential to practice and master before running. Marching can help improve running form and economy!
Single Leg Squats
Sample [P]rehab Running Program Exercise
Running is a single-leg sport, building adequate unilateral leg strength is a prerequisite to running!
Loaded Carries
Did you know running can produce forces up to 3-6X your body weight on your joints? Loaded carries are the perfect exercise to bridge the gap from low-impact to high-impact exercises to prepare your body for the large forces imposed by running.
Pogos
Sample [P]rehab Running Program Exercise
Ultimately you have exposed the involved bone and body area to impact for returning to running after a bone stress fracture. Pogos are a really nice way to introduce impact along with being easy to measure. You can keep track of total contacts with the ground, or keep track of how many rounds you did and for how long. For instance, you could start with 3 rounds of 30s and count how many times total you contact the ground. The goal would be to increase volume to a few sets performed 2-3x/day as bone remodeling does better with small bouts of loading dispersed throughout the day versus a lot of volumes done all at once. Allow for adequate recovery and bone remodeling to take place by taking off days as needed.
Easy To Follow Return To Running Protocol
When it comes time to run, the University of Delaware Return To Running Protocol is one we highly recommend. Two simple modifications with running that can also help with avoiding a BSI from occurring again are…
- Running ‘soft’ – think about making less noise with each step
- Increase step rate – increased step rate is associated with lower Ground Reaction Forces (GRF), which are basically the forces imposed on the body with running every time you make contact with the ground (3)
Be sure to follow the return to running rules as well as the soreness rules to get back to running after a bone stress fracture pain-free! You can also find another graduated running program to return a runner to 30 minutes of pain-free running by clicking HERE and looking at table 3.
LISTEN: MANAGING RUNNERS WITH CHRIS JOHNSON

Supplemental Blood Flow Restriction (BFR) protocol
Blood Flow Restriction Training (BFRT) is becoming a popular rehab tool for running after a bone stress fracture as there is evidence to support it can improve bone-specific metabolism (4). This is an especially favorable rehab tool as it allows individuals to perform resistance training at low loads (20-30% 1RM) or non-impact/low-impact aerobic exercise and still achieves significant muscle size gains, strength gains, and even cardiovascular gains. In previous times, typically someone with a bone stress injury or bone stress fracture would become deconditioned due to inactivity/rest prescribed by their doctor. Now we can mitigate the amount of muscle atrophy and deconditioning using BFRT within this golden window of opportunity.

Bone and cartilage tissue are similar in ways to muscle, if you don’t use it you lose it! Unfortunately, being non-weight-bearing and on physical rest does not stimulate bone optimally. As much as we need to protect the bone to let it heal, if we can find a way to stimulate the bone safely such as using a technique like BFR, we can help speed up recovery times. This can set people up for success when it comes time for graded exposure to high-impact physical activities such as running after a bone stress fracture.
Below you will find a BFR protocol we have designed for rehab from bone stress injuries and bone stress fractures. This is a rough outline along with exercise ideas and progressions that we have used in the clinic. It is important you consult with a healthcare professional and get clearance from your physician prior to participating in this protocol.
*For healthcare professionals – it is ok to extend and/or delay phases based on the injury site and risk profile, time period of immobilization and/or non-weight-bearing, and response/tolerance to exercise progressions. This should be looked at as a flexible guide to help you manage runners with BSI or bone stress fractures, not hard rules*
Return To Running After a Bone Stress Fracture: Phase 1
(Weeks 0-2) OR once the individual is cleared/appropriate for BFR. The typical scenario will be immediately after injury AND the individual is not mobile/non-weight bearing and cannot tolerate isolated/open-kinetic-chain resistance training with light loads (BW-40% 1RM).
Cell Swelling Protocol – 80% LOP determined using a doppler, 5 minutes on, 3 minutes off, up to 5 rounds, and can be performed 1-2x/day for 5-6 days a week
- Session 1 – Two to three rounds of cell swelling with focused isometrics as tolerated, otherwise passive or with e-stim (3s contract, 1s relax) I.E., if femoral shaft stress fx – perform quad sets OR in foot/ankle complex – perform isometric plantarflexion by pulling the foot into dorsiflexion with a resistance band but not letting the foot move.
- Session 2 – Three to four rounds of cell swelling with the same parameters above
- Session 3 and on until performing isolated/CKC/compound exercises – perform 5 rounds of cell swelling with the same parameters above
2-3x/week Biking Protocol – An option if the non-weight-bearing period is extended (3 or more weeks) and biking is OK. This would replace the cell swelling protocol.
- Bilateral BFR is better than unilateral for more cardiovascular adaptations, however unilateral on the affected side is appropriate
- Session 1 – Perform 1-2 rounds of biking for 5 minutes at 40% Heart Rate Reserve (HRR), if the individual is deconditioned or having difficulty you can decrease to 30-35% HRR. The occlusion is continuous while biking with at least 1 minute of deflate/free flow between rounds.
- Session 2 – Perform 1 round of biking for 10 minutes or as tolerated at the same HRR as session 1, the occlusion is continuous while biking
- Session 3-4 – Work towards 15 minutes total of biking, which can be continuous or with multiple rounds (I.E., 3 rounds of 5 minutes), at least 1 minute of deflate/free flow between rounds. Increase HRR by 5% from Session 2.
- Session 5 and on – Increase biking volume and intensity working towards 20 minutes of continuous biking at 50% HRR with ideally 80% LOP occlusion. Increase HRR by 5% each week until you reach 50%.
Return To Running After a Bone Stress Fracture: Phase 2
(Weeks 2-6) OR once the individual is weight-bearing and can tolerate isolated/open-kinetic-chain resistance training with light loads (BW-40% 1RM)
- 2x/week – BFR with treadmill walking at 60-80% LOP
- Bilateral BFR is better than unilateral for more cardiovascular adaptations, however unilateral on the affected side is appropriate
-
- To hit target training HR, increase incline if needed after reaching 3.5-3.7 MPH, limit an individual to brisk walking only vs. jogging/running.
-
-
- Session 1 – Perform 1-2 rounds of walking for 5 minutes at 40% Heart Rate Reserve (HRR), if the individual is deconditioned or having difficulty you can decrease to 30-35% HRR. The occlusion is continuous while walking with at least 1 minute of deflate/free flow between rounds.
-
-
-
- Session 2 – Perform 1 round of walking for 10 minutes or as tolerated at the same HRR as session 1, the occlusion is continuous while walking
-
-
-
- Session 3-4 – Work towards 15 minutes total of walking, which can be continuous or with multiple rounds (I.E., 3 rounds of 5 minutes), at least 1 minute of deflate/free flow between rounds. Increase HRR by 5% from Session 2.
-
-
-
- Session 5 and on – Increase walking volume and intensity working towards 20 minutes of continuous walking at 50% HRR with ideally 80% LOP occlusion. Increase HRR by 5% each week until you reach 50%.
-
- 2x/week on separate days from the BFR treadmill program – BFR with progressive resistance training at 60-80% LOP
- Bilateral BFR if desired for more systemic effects and training on the other side, however unilateral on the affected side is appropriate
- Exercise parameters are 30/15/15/15 reps with 30s breaks between each block of reps, and continuous occlusion for the entire 75 reps. 1 minute of rest and deflate/free-flow between each exercise.
- Sample progressive program below – general rules are starting with isolated/non-weight bearing exercises and progressing towards closed-kinetic-chain and upright/weight-bearing exercises
- Bilateral BFR if desired for more systemic effects and training on the other side, however unilateral on the affected side is appropriate
-
- Session 1
- Double Leg Bridge with the band above knees
- Clams with the band above knees
- LAQs with a band around ankles or ankle weight
- Long sitting ankle PF with band
- Session 1
-
-
-
- Session 2
- Double Leg Bridge with the band above knees
- side-lying hip abduction (with a band above knees if tolerated)
- LAQs with a band around ankles or ankle weight
- Loaded Seated heel raises
- Session 2
-
-
-
-
-
- Session 3
- Bodyweight squats with a band above the knees
- Standing heel raises
- Staggered stance Bridge with a band above knees
- LAQs with a band around ankles or ankle weight
- Loaded Seated heel raises
- Session 3
-
-
-
-
-
- Session 4
- Staggered bodyweight squats with a band above knees
- Anterior step-up
- Loaded Standing heel raises
- Staggered stance Bridge with a band above knees
- Leg extensions @ 20% 1RM
- Session 4
-
-
-
-
-
- Session 5
- Loaded anterior step-up
- Single Leg heel raises
- Loaded goblet squats with a band above knees
- Single-Leg Bridge with a band above knees
- Leg extensions @ 25-30% 1RM
- Session 5
-
-
-
-
-
- Session 6
- Posterior step-down
- Loaded Single leg heel raises
- Split Squat
- Loaded Farmer Carry
- RDL bodyweight
- Session 7
- TRX single-leg squat
- Split Squat
- Loaded Single leg heel raises
- Loaded Farmer Carry on toes
- RDL with weight
- Session 6
-
-
-
-
-
- Session 8 and on
- Strength training with the progressive overload principle
- Continue to integrate more planes of motion and unilateral work
- Continue to progress axial loading while targeting the specific affected tissue
- Move away from BFR and towards high-load resistance training (>65% 1RM) once tolerated
- Introduce progressive plyometrics when appropriate in preparation for graded exposure return to running
- Landing drills
- Pogos
- Jogging in place
- Skipping
- Session 8 and on
-
-
Return To Running After A Bone Stress Fracture: Phase 3
(Weeks 6+) OR once the individual has started a graded exposure return-to-running protocol
- 1x/week – BFR with treadmill walking at 60-80% LOP
- Working towards 20 minutes of continuous walking at 50% HRR with ideally 80% LOP occlusion
- 1x/week on separate days from the BFR treadmill program – BFR with progressive resistance training at 60-80% LOP
- Working towards 5 closed-chain compound axial loading exercises while targeting the specific affected tissue
- When high-intensity resistance training (HIRT) is tolerated (>65% 1RM) symptom-free, replace BFR with HIRT for at least 2 sessions/week while running on opposite days.
Closing Thoughts
Early management including a proper diagnosis and treatment plan is crucial for stress fractures. If you happen to be experiencing pain while performing a specific activity that is increasing in intensity and becoming more frequent, be sure to stop that activity and seek medical consultation. When returning to running after a bone stress fracture, there is a systematic approach to building your body back up to its optimal capacity, ultimately ensuring you will be able to return to your prior level of function even better than ever!
Maximize Your Running Performance

The human movement system provides a beautiful example of a build meant for movement efficiency. The tendons are built not just to anchor down muscles, but also to store and release energy acting as a spring to propel us forward. We were built to run, and not just to run, but to run gracefully. That script can for sure change when muscle weakness is present, tendon elastic energy is lost, or an injury occurs. No worries, running efficiency will return by completing this program!
References
- Tenforde AS, Kraus E, Fredericson M. Bone stress injuries in runners. Phys Med Rehabil Clin N Am. 2016;27(1):139–49.
- Pegrum J, Crisp T, Padhiar N. Diagnosis and management of bone stress injuries of the lower limb in athletes. BMJ 2012;344:e2511.
- Warden SJ, Davis IS, Fredericson M. Management and prevention of bone stress injuries in long-distance runners. J Orthop Sports Phys Ther 2014;44:749–65.
- S. T. Bittar , P. S. Pfeiffer, H. H. Santos and M. S. Cirilo-Sousa. Effects of blood flow restriction exercises on bone metabolism: a systematic review. Clin Physiol Funct Imaging (2018). doi: 10.1111/cpf.12512
About The Author
Craig Lindell, PT, DPT, CSCS
[P]rehab Co-Founder & Chief Content Officer
 Craig was born and raised in Blackwood, New Jersey, and grew up with a passion for sports. Craig played soccer at a competitive level through high school. Craig found interest in physical therapy as a career after experiencing it first-hand due to a quadriceps injury. Because of this exposure, Craig went on to college at Pennsylvania State University to pursue his Bachelor of Science degree in Kinesiology with a focus in Movement Science. Craig has experience with athletes at the D1 level as he worked with Penn State Women’s soccer team. After undergrad, Craig packed his bags and drove to California to pursue his Doctor of Physical Therapy at the University of Southern California. In his spare time, Craig enjoys golfing, hiking, traveling, and spending time with his wife and dog. Craig has a special interest in helping younger athletes with adolescent athletic development and working with soccer players, golfers, and individuals going through ACL rehab.
Craig was born and raised in Blackwood, New Jersey, and grew up with a passion for sports. Craig played soccer at a competitive level through high school. Craig found interest in physical therapy as a career after experiencing it first-hand due to a quadriceps injury. Because of this exposure, Craig went on to college at Pennsylvania State University to pursue his Bachelor of Science degree in Kinesiology with a focus in Movement Science. Craig has experience with athletes at the D1 level as he worked with Penn State Women’s soccer team. After undergrad, Craig packed his bags and drove to California to pursue his Doctor of Physical Therapy at the University of Southern California. In his spare time, Craig enjoys golfing, hiking, traveling, and spending time with his wife and dog. Craig has a special interest in helping younger athletes with adolescent athletic development and working with soccer players, golfers, and individuals going through ACL rehab.
Disclaimer – The content here is designed for information & education purposes only and is not intended for medical advice.
About the author : Craig Lindell PT, DPT, CSCS
Related posts




Latest Blogs





