


Playing in numerous sports throughout my life it seemed the response to injury was pretty much the same, put some ice on it, and RICE (Rest, ICE, Compression, Elevation). However, it felt like there was no real rhyme or reason to this decision, that’s just what the coaches said to do! For the past three years, I’ve had the opportunity to provide sideline coverage as a sports physical therapist ranging from youth up to professional sports. Part of this job description is carrying an ice chest from the parking lot to the fields/stadium that typically seems to be uphill and miles away. During this walk, including multiple breaks (the ice chest gets heavy!), I’ve asked the following: why do we rest, ice, compress, and elevate after an injury? Where did this originate? Is this still best practice? In this article, you’ll learn the truth about icing injuries and why we need to step away from RICE and move towards PEACE & LOVE.
When Did Icing Injuries First Begin?
Before we get into the truth about icing injuries, it’s storytime! The year is 1962 and a freckled-faced 12-year-old boy hops onto a freight car in Somerville, Massachusetts. Why? He’s a 12-year-old boy and it’s a dangerous game. The train rolls under a bridge and the boy, Everett Knowles, doesn’t hug the ladder rail tight enough. This results in his arm being almost completely severed from his body. He is rushed to the hospital where, for the first time in history, Dr. Ronald Malt decides to surgically reattach the arm. In the process of assembling the dream team for the surgery, he orders the arm to be preserved by placing it in ice. The surgery takes about 15 hours and is a success.
Following this success, Dr. Malt and his team travel around the world explaining the surgery. In a press conference a reporter asks “if we encounter a person with a severed arm, what should we do?” He replies, “Don’t panic, place the limb on ice, stop the bleeding by using a tourniquet, and elevate it above the heart.” This then becomes known respectively as rest, ice, compress, and elevate. The term is coined and introduced into sports medicine by Dr. Robert Mirkin in his bestselling The Sportsmedicine book in 1978. From 1978 to the present day, RICE is the most widely used principle for acute/initial injuries.
To Ice Or Not To Ice?
Why Do We Use The RICE Principle?
In order to understand the proposed theory of why this principle is used, we’re going to have to take a deep dive into the basic physiology of acute musculoskeletal injury. The initial response is a complex immune response with the goal of “attack.” For a very, very, very detailed description of this process please see Tidball’s 2017 paper. In this phase, vasoconstriction occurs to stop bleeding and various white blood cells go to the area to eliminate the invader. During the process, secondary damage is likely done to the area. The second part of the initial inflammatory phase is characterized by vasodilation to bring blood to the area and “rebuild” or “regenerate”. It is important to note that both of these inflammatory responses are necessary for healing to occur. The effects of the inflammatory phase result in redness, swelling/edema, hypersensitivity, and nociception. We are just going to call this “congestion.” The RICE principle is thought to decrease the congestion and decrease inflammation to help recover from an injury.
READ: HOW TISSUE HEALING WORKS
Is RICE Still Best Practice? The Truth About Icing Injuries
…No. Inflammation isn’t the bad guy and actually, it’s NEEDED for healing to occur. Remember Dr. Mirkin? He coined the term RICE in 1978, but recently he has written, “Coaches have used my ‘RICE’ guideline for decades, but now it appears that both ice and complete rest may delay healing, instead of helping.” I applaud his ability to change his perspective based on the best available evidence in the present time and update us on the truth about icing injuries. Let’s dive into this topic a bit deeper.
Have You Just Suffered A Hamstring Injury?

Hamstring injuries can be straightforward or can disguise themselves as false sciatic pain or piriformis syndrome. In either case, the solution becomes the same: an early movement that protects the area while creating enough of a stimulus to become stronger!
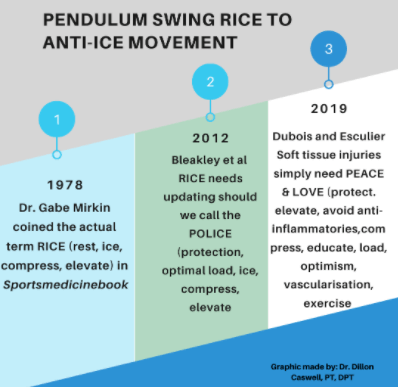
Pendulum Swing: RICE To Anti-Ice Movement
When an acute musculoskeletal injury occurs we want to first rule out any fractures, dislocations, or anything else that would require referral for emergency medicine. Next, we want to decongest the congested area. In order for this to happen, we have to utilize the lymphatic system. This system is a collective of vessels and organs that relies mostly on extrinsic pumping of skeletal muscle and breathing to rid our bodies of waste, toxins, and extra fluid.
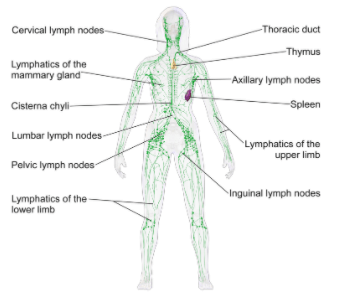
Compression may help to reduce swelling but muscle contraction is more beneficial due to pressure differences. For example, most compression garments have a pressure of approximately 30-40 mmHg, whereas contraction of the calf causes approximately 200 mmHg of pressure on the local veins. This is also why absolute rest is not likely the best practice after an injury. Muscular contraction and breathing are needed to decongest the area; maybe the classic “walk it off” coaching comment wasn’t the worst advice! Movement stimulates healing through the process of mechanotransduction. Elevation may also still be done, however, this is supported by weak evidence and is more recommended due to the low risk-benefit ratio. That covers the R, C, and E of RICE, but I want to know the truth about icing injuries and if I need to keep carrying this heavy ice chest to games!
LISTEN: CORTISONE SHOTS WITH DR. ALEX WEBER

Ice was recommended to be used for proposed anti-inflammatory benefits. This is very true for ibuprofen, which is significantly overused by our youth athletes. As stated above, we want inflammation to occur as it is necessary to begin the healing process. Recent research has shown anti-inflammatory medications and ice may be detrimental for long-term tissue healing. Ice is commonly used in baseball after pitching. Currently, 10/30 MLB teams no longer ice their pitchers after an outing. Research done by Tseng et al. 2013 found signs of muscle damage after applying topical cooling following eccentric exercise compared to a sham application. Furthermore, a randomized controlled trial by Prins et al. 2011 tested the effectiveness of ice therapy in the initial phases of a calf muscle tear. They compared two groups, active ice group vs control group, and looked at functional capacity, time to return to work, and pain relief. They concluded, “the use of ice is not beneficial for people receiving ice therapy.” It is important to point out that the research on ice/cryotherapy has its methodological flaws (you either know it’s ice or it isn’t…), so we don’t conclude anything with full certainty.
Why, then, can ice still seem to help with pain? The benefits of ice likely lie in the fact that most people believe that it is going to make them feel better. It is unlikely that an ice pack is reaching depths to truly make a physiological change at the injury site. Bleakley and Hopkins 2013 stated “Based on healthy human models, it is difficult to induce large decreases in intramuscular or joint temperature, particularly in circumstances of deep tissue injury or areas of higher levels of body fat. The lowest reported superficial muscle temperature (1 cm sub-adipose) after cryotherapy is 21°C, in a lean athletic population. Reaching currently accepted threshold temperatures for metabolic reduction (5–15°C) seems unlikely.” It is likely that the superficial treatment of ice causes a change in our nervous system sensitivity leading to the perception of the injured area feeling better. You can learn more about this theory here.

The Prehab membership is the anti-barrier solution to keeping your body healthy. Access state-of-the-art physical therapy, fitness programs, and workouts online in the comforts of your own home or gym! Taking control of your health with exercise & education from the palm of your hand has never been easier. Get access to 50+ programs, 100+ unique workouts, and 3000+ exercises to build your own workout routines. Trial it for free, and learn how to get out of pain, avoid injury, and optimize your health with [P]rehab!
So Then, What Is Considered Best Practice For Acute Musculoskeletal Injury?
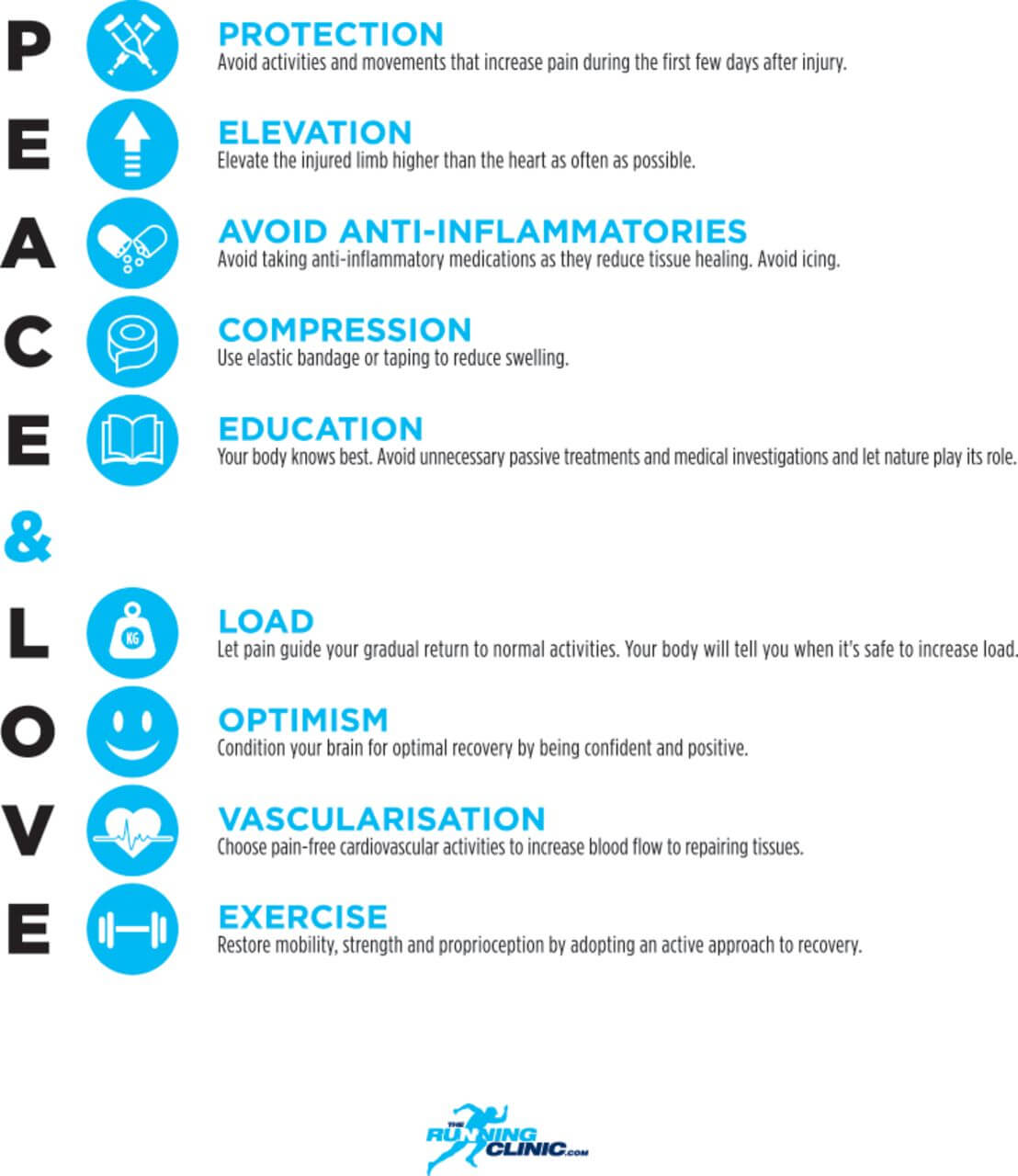
The RICE principle has transitioned from RICE to PRICE to POLICE to now PEACE & LOVE
Finally, the truth about icing injuries! We will outline what we now use for athletes of all ages when an acute injury occurs:
- Rule out any condition requiring referral to the hospital. If no referral is needed, let the athlete know this information to create safety and decrease fear or uncertainty (example video below in regards to ankle fracture).
READ: DO I NEED AN X-RAY AFTER AN ANKLE SPRAIN?

- Assess immediate tolerance to load and identify the optimal load. The optimal load is dependent on symptom response. Can they lightly move the injured area without weight being put onto it? If yes, then how much weight can be put through the injured area? Can the athlete walk, limp, or are they not accepting any load through the area?
- Do they have hopes to return to play within the same day? If yes, then I’m not going to use ice. Research has shown the application of ice for greater than five minutes decreases strength, power, and performance in the short term. If ice is used, then a period of rewarming is needed before the athlete proceeds into higher-level movements. Instead, we will use optimal load and progress this load until the athlete feels confident with a quick screen on the sideline of sport-specific demands (running, jumping, absorbing contact, etc)
- If the athlete communicates that they do not want to return to play within the same day, we move to pain-free exercise followed by compression, elevation, education, avoiding anti-inflammatory medications, and ice (if they REALLY want it).
Learn how to better use heat & cold therapy for pain & injuries
Closing Thoughts
Our goal is to introduce safe movements to our youth athletes after their first injury experience, allowing them to learn that movement and perspective made them better – not ice. In the future, we hope to only use ice for cases of heat exhaustion. Therefore, we conclude the truth about icing injuries and the effectiveness of ice for acute musculoskeletal injury is due to the belief it will help, changes in sensory nerve conduction, and the ability for ice to melt and become water to hydrate the athlete.
Take Care of Your Hamstring Issues

Hamstring injuries can be quite frustrating, especially if not treated the right way early on. Take care of your hamstring issues today!
References
- Available at: https://www.thesomervilletimes.com/archives/36886
- Available at: https://www.drmirkin.com/fitness/why-ice-delays-recovery.html
- Tidball JG. Regulation of muscle growth and regeneration by the immune system. Nat Rev Immunol. 2017;17(3):165-178.
- Smith C, Kruger MJ, Smith RM, Myburgh KH. The inflammatory response to skeletal muscle injury: illuminating complexities. Sports Med. 2008;38(11):947-69.
- Moore JE, Bertram CD. Lymphatic System Flows. Annu Rev Fluid Mech. 2018;50:459-482.
- Tseng CY, Lee JP, Tsai YS, et al. Topical cooling (icing) delays recovery from eccentric exercise-induced muscle damage. J Strength Cond Res. 2013;27(5):1354-61.
- Singh DP, Barani Lonbani Z, Woodruff MA, et al. Effects of topical icing on inflammation, angiogenesis, revascularization, and myofiber regeneration in skeletal muscle following contusion injury. Front Physiol2017;8: 93.
- Prins JC, Stubbe JH, Van meeteren NL, Scheffers FA, Van dongen MC. Feasibility and preliminary effectiveness of ice therapy in patients with an acute tear in the gastrocnemius muscle: a pilot randomized controlled trial. Clin Rehabil. 2011;25(5):433-41.
- C. M. Bleakley & J. T. Hopkins (2010) Is it possible to achieve optimal levels of tissue cooling in cryotherapy?, Physical Therapy Reviews, 15:4, 344-350,
- Esperanza Herrera, Maria C. Sandoval, Diana M. Camargo, Tania F. Salvini, Motor and Sensory Nerve Conduction Are Affected Differently by Ice Pack, Ice Massage, and Cold Water Immersion, Physical Therapy, Volume 90, Issue 4, 1 April 2010, Pages 581–591
- Bleakley CM, Glasgow PD, Phillips N, et al. Guidelines on the management of acute soft tissue injury using protection rest ice compression and elevation. London: ACPSM, 2011.
- Bleakley CM, Glasgow P, MacAuley DC. Price needs updating, should we call the police? Br J Sports Med2012;46: 220-1.
- Doherty C, Bleakley C, Delahunt E, et al. Treatment and prevention of acute and recurrent ankle sprain: An overview of systematic reviews with meta-analysis. Br J Sports Med2017;51: 113-25.
- Duchesne E, Dufresne SS, Dumont NA. Impact of inflammation and anti-inflammatory modalities on skeletal muscle healing: From fundamental research to the clinic. Phys Ther Sport2017;97: 807-17.
- Hansrani V, Khanbhai M, Bhandari S, et al. The role of compression in the management of soft tissue ankle injuries: A systematic review. Eur J Orthop Surg Traumatol 2015;25: 987-95.
- Khan KM, Scott A. Mechanotherapy: How physical therapists’ prescription of exercise promotes tissue repair. Br J Sports Med2009;43: 247-52.
- Blaise Dubois et al.,Soft tissue Injuries simply need PEACE & LOVE British Journal of Sports Medicine, 2020 Khan KM, Scott A Mechanotherapy: how physical therapists’ prescription of exercise promotes tissue repair British Journal of Sports Medicine 2009;43:247-252.
About The Author
Dillon L Caswell, PT, DPT, SCS
[P]rehab Program Manager & Podcast Host
 Dillon is a Sports Physical Therapist, performance coach, and adjunct professor residing in Syracuse, NY whose passion is providing holistic solutions to improve all aspects of human performance. Along with working with clinical athletes across the lifespan, he provides on field coverage for youth and semi-professional teams. After his undergraduate studies at Syracuse University, he earned his Doctorate in Physical Therapy from SUNY Upstate Medical University, where he now serves as an Adjunct Professor. He is the founder and owner of AP3T: Action Potential Performance Physical Therapy practicing wellness, prevention, and solution-based health care. In his free time, he enjoys family dinners, playing with his dog, and competing as a CrossFit athlete. Dillon honors the opportunity to join the [P]rehab guys to influence and educate in a people first system!
Dillon is a Sports Physical Therapist, performance coach, and adjunct professor residing in Syracuse, NY whose passion is providing holistic solutions to improve all aspects of human performance. Along with working with clinical athletes across the lifespan, he provides on field coverage for youth and semi-professional teams. After his undergraduate studies at Syracuse University, he earned his Doctorate in Physical Therapy from SUNY Upstate Medical University, where he now serves as an Adjunct Professor. He is the founder and owner of AP3T: Action Potential Performance Physical Therapy practicing wellness, prevention, and solution-based health care. In his free time, he enjoys family dinners, playing with his dog, and competing as a CrossFit athlete. Dillon honors the opportunity to join the [P]rehab guys to influence and educate in a people first system!
Disclaimer – The content here is designed for information & education purposes only and is not intended for medical advice.
About the author : Dillon Caswell PT, DPT, SCS
9 Comments
Leave A Comment
You must be logged in to post a comment.
Related posts




Latest Blogs

Get Proactive with Prehab
- ✔ Zero wait times, no hidden fees, no barriers to entry!
- ✔ Get out of pain, get stronger, and improve your mobility
- ✔ Access to easy-to-digest physical therapy education videos & resources to learn about your body in the palm of your hand
- ✔ Guidance from trusted Doctors of Physical Therapy







Every time I read one of your articles like this I just want to stand up and applaud. Educating=Empowering and you’re doing that for people.
These articles are like sitting down to a gourmet meal versus finding a recipe, shopping for all the ingredients, measuring, prepping, mixing, assembling them all together, tweeking what doesn’t work, trying again…… Thank you guys so much for assembling all this information in an easily digestible form for everyone (and for including links for some of us geeks who want to dive deeper..
Keep the great info coming. Appreciate you guys!
Hey Danielle! Thank you so much for reading and for your comment! We cannot agree that edcuating is empowerment! And we hope that many people can read this information as much as possible and share it so we can better educate the world!
Didn’t see a reference to Mirkins retraction of RICE and the damage it caused. Any reason?
Hey Coach, Thank you for reading the article! The reference for the Mirkins retraction is listed in references 2.) Available at: https://www.drmirkin.com/fitness/why-ice-delays-recovery.html. My apologies for not linking it in the paper!
I applaud your well thought, in depth analysis of this topic. I miss the days of authors who present facts and data then let the conclusions draw themselves. I too have been preaching the unreliable merits of ice, based on tradition not data, and have been met with much eye rolling. I hope people take the time to appreciate the evidence you provided but fear that they won’t take the time to read it…it’s much easier to tweet an opinion these days than to provide data which promotes meaningful conversation
Keep fighting the good fight
Phil C, MPT
Thank you so much for your positive support and thoughtful response! Best of luck to you and your continued practice :).
Of course, best of luck to you as well!
Thanks for this article. I’m so glad that the “call the POLICE” metaphor phase was brief…
Could you write an article about inflammation? I’m specifically trying to understand inflammation and edema in and around a knee, post injury. How important is it to really work on reducing it, how much does it interfere with regaining flexion and terminal extension, and strategies for managing it, especially if RICE + NSAIDS is not necessarily the best plan. Does it eventually just go away as long as you’re making progress regaining strength and mobility? Or do you have to play an active part in ensuring it resolves? Ice or heat? Dry or moist heat?
Thank you for what you do!
Hi Carrie, Thank you for reading and for the comment! Love that idea as an article topic!!! To answer briefly here, it can play a big role in limiting range of motion post-op. The initial inflammation is a beautiful thing as it starts the healing cascade, the byproducts that are leftover “the chemical soup” is what we would want to get out of the area. Generally, the body will clear this out when it’s ready. To assist in that, movement is going to be the best agent, whereas modalities heat/ice likely do not help in that process with the exception of making the person more comfortable via sensory theory. Let us know if any further questions come up!!!