

On this page 6 sections
Your guide
What you'll learn
Nearly everyone has heard of the term Plantar Fasciitis. In popular culture, any kind of foot pain is often lumped in with the loose term plantar fasciitis. On the other hand, its lesser-known cousin, posterior tibial tendinopathy is rarely discussed in conversations amongst non-clinicians. Both, however, are common causes of foot pain. These two diagnoses present with many similarities and in very similar populations. Although there is much overlap between these two diagnoses there are several important differences. This article with highlight the unique characteristics of each diagnose as well as successful treatments for both.
What is Plantar Fasciitis?
Plantar Fasciitis is an irritation of the plantar fascia that is located on the bottom of the foot. The plantar fascia is a thick band of fibrous tissue connecting the heel bone to the toes. While plantar fasciitis was originally believed an inflammatory condition, recent evidence has suggested that inflammation is not the primary issue in plantar fascia. Thus, many in the medical community have begun using the term “plantar heel pain” (PHP). Plantar fasciitis or PHP is better described as a degeneration of the plantar fasciitis which includes microscopic tearing or fraying rather than an inflammatory condition. It should be noted that inflammation may present as your body tries to heal this degeneration but it is not the primary issue.

Thus, plantar fasciitis results from excessive loads being placed across the plantar fascia, leading to tissue degeneration. The plantar fascia is generally more stressed in weight-bearing situations, particularly when the foot is forced into a flatter or more pronated position.
Plantar fasciitis is therefore a condition of load mismanagement.
What is Posterior Tibialis Tendinopathy?
The posterior tibialis is a muscle that originates in the shin and travels behind the medial ball of your ankle, under and across your foot to insert on the lateral bones of the foot. Thus its primary role is to support the arch of your foot in weightbearing. As you take a step and land, your foot flattens out and your posterior tibialis is working overtime to control this flattening of your arch. Then as you go to push off that same foot, your tibialis posterior helps create a more rigid arch in your foot for you to push off of. This flattening of the foot is completely normal during the gait cycle and thankfully, we have the posterior tibialis tendon there to help to control this motion. Posterior tibialis tendinopathy is painful degeneration along the posterior tibialis tendon.
While the posterior tibialis tendon is a much more dynamic structure than the plantar fascia, in much the same way that PHP results from excessive loads across the plantar fascia, PTT results from excessive loads across the posterior tibialis tendon.
Thus posterior tibialis tendinopathy is also a condition of load mismanagement.

How Does Posterior Tibialis Tendinopathy Differ from Plantar Fasciitis?
The key difference between these two conditions lies in the irritated structures. In PTT it is the actual tendon that is working to support the arch that is irritated and painful whereas with PHP it is the plantar fascia that is being excessively loaded. The plantar fascia is a less dynamic structure than the posterior tibialis tendon and is not something that you can work on directly, whereas you can load and train your posterior tibialis tendon.

This leads to some key differences in the presentation of the two conditions. PTT often presents with pain higher up along the medial aspect of the foot and ankle whereas PHP often presents more along the bottom surface of the foot, usually closer to the heel. The hallmark sign of PHP is pain with the first few steps in the morning or after a period of prolonged sitting, although this can be present with PTT. A hallmark sign of PTT is decreased endurance and strength when performing single-limb heel rises, as well as the potential reproduction of pain.
Another key difference is in some of the treatment options for short-term pain relief in PHP. Soft tissue massage and stretching of the calf muscles and plantar fascia itself are "A level" recommendations in the PHP clinical practice guidelines, whereas they have little to no efficacy in PTT. Additionally, night splints and foot taping also have a prominent role in reducing stress across the plantar fascia in early rehab, whereas they are not highly recommended treatments for PTT. These differences in short-term treatment relate to the differences in the actual structures that we are trying to reduce the loads through to provide relief.
How Are Posterior Tibialis Tendinopathy and Plantar Fasciitis Similar?
Although they are conditions that involve different structures, PTT and PHP have a LOT in common. Most notably they are both conditions that result from a mismanagement of the loads through the foot. For both issues, the structures that support your foot in a healthy arch are being worked beyond their capacity leading to issues. One of these key structures is your posterior tibialis tendon which is the primary supporter of weight-bearing supination (or maintenance of a healthy arch).
For this reason, both conditions affect similar groups across a continuum. In one category they affected the young and physically active, like a runner who increased their mileage too quickly without giving their body the time to adapt to the increased loads. On the other hand, they affect the old and sedentary muscular deconditioning and increased body weight leads to increased stress across these structures.
In either case, the treatment plan is very similar, you must recondition the structures that support your arch and modify the irritating activities before gradually re-progressing it. For the young athlete, this may require dialing back their running program and for the older sedentary individual, this may mean losing weight. In both cases, the use of a pain monitoring scale where you limit activities that lead to increased pain afterward but allow yourself to perform activities with low-level pain that dissipates by the next day.
READ: PLANTAR FASCIITIS EXERCISES

What is important here is that, in both cases the treatment is not simply rest and activity modification, you must start to increase the workload tolerance of these structures. This means progressing up toward high-load strengthening, whether running marathons or simply spending a few hours on your feet, your plantar flexors and intrinsic foot muscles work hard to support your foot posture throughout the day and you must train them to do this.
Some foundational exercises include weighted single-leg heel rises, working your way of the rep schemes as high as 25-30 to build the endurance of your plantar flexors and allow your tendon to adapt to prolonged loading.
Exercise 01 of 03
Exercise demonstration
Single Leg Heel Raise Off Step

View exercise instructions
- HOW: Place a step in front of a wall or an object to use for balance. Using only one leg, step onto the box with the balls of your feet on the edge of the box, and let your heel hang off the box. While keeping your glutes and quads tight to keep your knee straight, lift your heel up in a slow and controlled manner, then slowly lower your heel back down to the ground. Repeat
- FEEL: You should feel your calf getting a workout, but also your glutes and quads working as well to help keep your leg straight.
- COMPENSATION: Do not let your knee bend as that is a different exercise. Make sure you go through your full range of motion at your ankle. This is not a balance exercise, so hold onto something to help with balance as the goal of this exercise is to strengthen your calf!
Single-leg balance exercises with a focus on maintaining the arch in your foot also will prepare you to do this during activities like walking and running.
Exercise 02 of 03
Exercise demonstration
Single Leg Short Foot Hold - Band

View exercise instructions
- HOW: Get set up standing with a theraband under the knuckle of your big toe on one side. Begin the exercise by lifting your arch and assuming optimal foot/ankle position, then balance on that leg for that time prescribed.
- FEEL: You should feel all the muscles in your foot, your arch, and your calf working with this exercise. After some time passes, you may also feel your hip on the same side you're balancing on working as well.
- COMPENSATION: Do not lose optimal foot/ankle position, don't let your arch fall, don't let the knuckle of your big toe lift off the ground. Maintain single leg balance with optimal pelvis and trunk control/position.
TheraBand resisted foot adduction also has been shown to selectively work the tibialis posterior and to help reduce pain in those with PTT. We also love this variation of the heel raise with the ball squeeze as squeezing the ball helps to further recruit the posterior tibialis muscle as it works to control the arch.
Exercise 03 of 03
Exercise demonstration
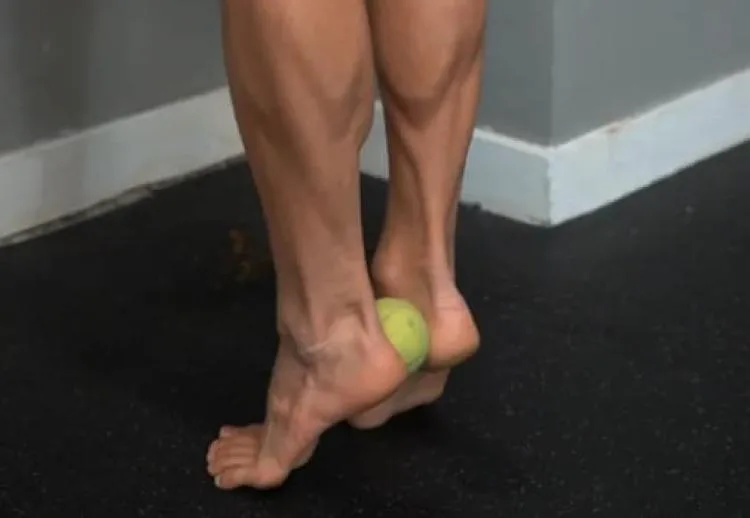
Heel Raise – Ball Squeeze
View exercise instructions
- HOW: Place a tennis ball, lacrosse ball, or any other small circular like object in between your heels. Squeeze the ball with your heelas and keep that constant tension during the whole exercise. Then, push up with your toes raising your heels. Make sure to push straight up with all of your toes working simultaneously. The goal is to keep the ball between your heel the entire time.
- FEEL: You should feel your calf muscles working.
- COMPENSATION: Don’t let go of the ball as you raise your heels. Control the motion and do not go too fast.
Closing Thoughts:
While PTT and PHP are different conditions that involve the exacerbation of different structures in different areas of the foot, their treatment and causes are very similar. In both cases, they result from a mismanagement of the loads across the foot, specifically those that lead to the collapsing of the healthy arch in your foot. Treatment for both of these conditions requires a temporary decrease in the stress in the offending area, often by limiting irritating activity using a pain monitoring scale and providing some arch support when appropriate, as well as training the structures that support your arch to tolerate higher loads. This training should include progressively overloaded close-chain foot adduction, plantar flexion, and single-leg stance activities.
LEARN MORE ABOUT OUR PLANTAR FASCIITIS REHAB PROGRAM
References:
- KULIG, KORNELIA1; BURNFIELD, JUDITH M.1,2; REQUEJO, SUSAN M.1; SPERRY, MICHELLE1; TERK, MICHAEL1. Selective Activation of Tibialis Posterior: Evaluation by Magnetic Resonance Imaging. Medicine & Science in Sports & Exercise 36(5):p 862-867, May 2004. | DO
- Kornelia Kulig, Stephen F Reischl, Amy B Pomrantz, Judith M Burnfield, Susan Mais-Requejo, David B Thordarson, Ronald W Smith, Nonsurgical Management of Posterior Tibial Tendon Dysfunction With Orthoses and Resistive Exercise: A Randomized Controlled Tria
- Allam AE, Chang KV. Plantar Heel Pain. [Updated 2022 Sep 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-.
- Morrissey D, Cotchett M, Said J'Bari A, et al. Management of plantar heel pain: a best practice guide informed by a systematic review, expert clinical reasoning, and patient values. Br J Sports Med. 2021;55(19):1106-1118. doi:10.1136/bjsports-2019-10197
- Ross MH, Smith MD, Mellor R, Durbridge G, Vicenzino B. Clinical Tests of Tibialis Posterior Tendinopathy: Are They Reliable, and How Well Are They Reflected in Structural Changes on Imaging?. J Orthop Sports Phys Ther. 2021;51(5):253-260. doi:10.2519/j
- Koc TA Jr, Bise CG, Neville C, Carreira D, Martin RL, McDonough CM. Heel Pain - Plantar Fasciitis: Revision 2023. J Orthop Sports Phys Ther. 2023;53(12):CPG1-CPG39. doi:10.2519/jospt.2023.0303
About the Author
Tommy Mandala, PT, DPT, SCS, OCS, CSCS
[P]rehab Writer & Content Creator
 Tommy Mandala is a Doctor of Physical Therapy, Board Certified Clinical Specialist in Sports & Orthopedics, and Certified Strength and Conditioning Specialist in New York City. He is the founder of ALL IN ACL, a digital coaching platform dedicated exclusively to helping ACLers return to the life they had before their injury with full confidence in their knee. Prior to that, he worked in the sports clinic at Hospital for Special Surgery, the #1 Orthopedic Hospital in the country. While there, he had the opportunity to hone his skills as an ACL specialist working closely with world renowned surgeons and evaluating patients from all over the world. He completed his sports residency training at the University of Delaware where he had opportunities to work with many of their Division I sports teams as well as the Philadelphia 76’ers NBA G-league affiliate, the Delaware Blue Coats. He also trained at Champion Sports Medicine in Birmingham, Alabama where he had the opportunity to learn from researchers in the American Sports Medicine Institute. Currently, Tommy works exclusively with ACLers through his digital coaching model. While many of these clients are athletes, Tommy works with ACLers of all different abilities helping them to build the strength they need to overcome this unique injury. One of his favorite aspects of his job is taking active clients who have never been a “gym person” before and showing them the amazing things that happen when they learn to strength train.
Tommy Mandala is a Doctor of Physical Therapy, Board Certified Clinical Specialist in Sports & Orthopedics, and Certified Strength and Conditioning Specialist in New York City. He is the founder of ALL IN ACL, a digital coaching platform dedicated exclusively to helping ACLers return to the life they had before their injury with full confidence in their knee. Prior to that, he worked in the sports clinic at Hospital for Special Surgery, the #1 Orthopedic Hospital in the country. While there, he had the opportunity to hone his skills as an ACL specialist working closely with world renowned surgeons and evaluating patients from all over the world. He completed his sports residency training at the University of Delaware where he had opportunities to work with many of their Division I sports teams as well as the Philadelphia 76’ers NBA G-league affiliate, the Delaware Blue Coats. He also trained at Champion Sports Medicine in Birmingham, Alabama where he had the opportunity to learn from researchers in the American Sports Medicine Institute. Currently, Tommy works exclusively with ACLers through his digital coaching model. While many of these clients are athletes, Tommy works with ACLers of all different abilities helping them to build the strength they need to overcome this unique injury. One of his favorite aspects of his job is taking active clients who have never been a “gym person” before and showing them the amazing things that happen when they learn to strength train.