
“Synovial Plica Syndrome.” That’s a mouthful of musculoskeletal jargon, isn’t it? It sure is. The plica isn’t nearly as well known by the public as other common sources of anterior knee pain like patellar tendinopathy or patellofemoral pain syndrome. Regardless, you’re probably here with us now because someone diagnosed you with it: Synovial Plica Syndrome. But what is a plica? Why is it hurting? And what can you do about it? Go ahead and read on; we’ve got you covered.
What is a plica?
Let’s take a few steps back first. We can’t really discuss the plica without first understanding some other anatomy. I want you to first imagine your knee joint, where your thigh bone (femur) connects to your shin bone (tibia).

Femur up top, tibia at the bottom. With me so far? Screenshot from Essential Anatomy 5. (3D4Medical, Elsevier.)
Now, as I’m sure you can appreciate, there are a ton of muscles, tendons, and ligaments that cross this joint, making sure it stays nice and stable. When you strip away all of this soft tissue you’re left with two capsular layers that create an encasement around the knee joint. The outermost layer is called the articular capsule, while the innermost layer is called the synovial membrane. In reality, these would have to be dissected carefully to dissociate from one another, but for the purpose of conversation, they should be discussed separately.
Maximize Your Rehab For Knee Plica Syndrome

The Knee Rehab Program is a physical therapist-developed, step-by-step program to help you minimize knee pain and optimize knee health. It will teach you how to build a strong foundation for your knees with lower body strengthening & stabilization exercises. Ultimately, our program is designed to bulletproof your knees to last a lifetime! Get started HERE.
The outermost layer, the articular capsule, is most commonly referred to as the joint capsule. It functions as a sac, enclosing the ends of your femur and tibia. This layer is fairly fibrous and tough.

The outermost layer, the articular capsule. Screenshot from Essential Anatomy 5. (3D4Medical, Elsevier.)
When you pull this layer away, you’re looking at the innermost layer, the synovial membrane. The synovial membrane is a loose layer of connective tissue, elastin fibers, and adipose tissue. Its primary function is to secrete synovial fluid, which bathes and circulates the inside of the joint. Due to these structures, the knee is identified as a synovial joint.

The innermost layer, is the synovial membrane. Like peeling back layers of an onion, visualize that this lies directly underneath the articular capsule once removed. Screenshot from Essential Anatomy 5. (3D4Medical, Elsevier.)
It’s a silly metaphor, but imagine the encasement that the capsule (the term we’ll use to refer generically to both the articular capsule and synovial membrane) creates around the knee joint as a snow globe. The capsule is your glass of the snow globe and the ends of your femur and tibia are within the globe as the display pieces. The fluid contained within the snow globe is your synovial fluid, and the snowflakes are nutrients.
If you’ve ever spent more than 5 minutes with a physical therapist, you may have heard the old saying: “motion is lotion.” It’s true. When you go for a bike ride or a walk around the neighborhood, imagine your snow globe being gently shaken, allowing the snowflakes and fluid to move around and bathe the inside of your joint. This is essentially one of the functions of the synovial joint found at your knee. In contrast, imagine someone with a painful knee who instead remains sedentary: their snow globe remains stagnant and the knee remains painful.
So what’s a plica? It’s a bit of an abstract concept. A plica is a membranous inward fold that is part of the synovial lining of the knee joint capsule. It’s considered to be a remaining trace of embryologic knee development (1). It is present in everyone, but some folks, for whatever reason, are blessed to have plicae that are more prominent (2). Some folks are genetically blessed with athleticism, others get cute dimples when they smile — but you were lucky enough to inherit some larger membranous folds of plicae. Thanks, mom and dad.
The leading theory suggests that in utero the knee is formed initially into three separate compartments (medial, lateral, and suprapatellar) which are separated by mesenchymal tissue (cells that are undifferentiated and haven’t decided who they want to be when they grow up). At some point, these layers fuse together and leave behind remnants of the compartment separating membranes (1). And thus, plicae are born.
Of note, there are 4 different types of synovial knee plicae including infrapatellar, mediopatellar, suprapatellar, and lateral (3). The most clinically relevant is the mediopatellar, which is often blamed for the development of synovial plica syndrome (1). Orthopedists and anatomists often debate whether the lateral plica exists. Nevertheless, take a look at the illustration below.
 Here’s an excellent illustration of a dissected knee joint to show the various knee plicae (1). The knee is bent here to 90 degrees and the knee cap has been lifted up and away (you’re looking at the undersurface of it.) What we’re focusing in on is the “medial parapatellar plica,” or simply the mediopatellar plica. It’s the most clinically relevant and frequently blamed for synovial plica syndrome.
Here’s an excellent illustration of a dissected knee joint to show the various knee plicae (1). The knee is bent here to 90 degrees and the knee cap has been lifted up and away (you’re looking at the undersurface of it.) What we’re focusing in on is the “medial parapatellar plica,” or simply the mediopatellar plica. It’s the most clinically relevant and frequently blamed for synovial plica syndrome.
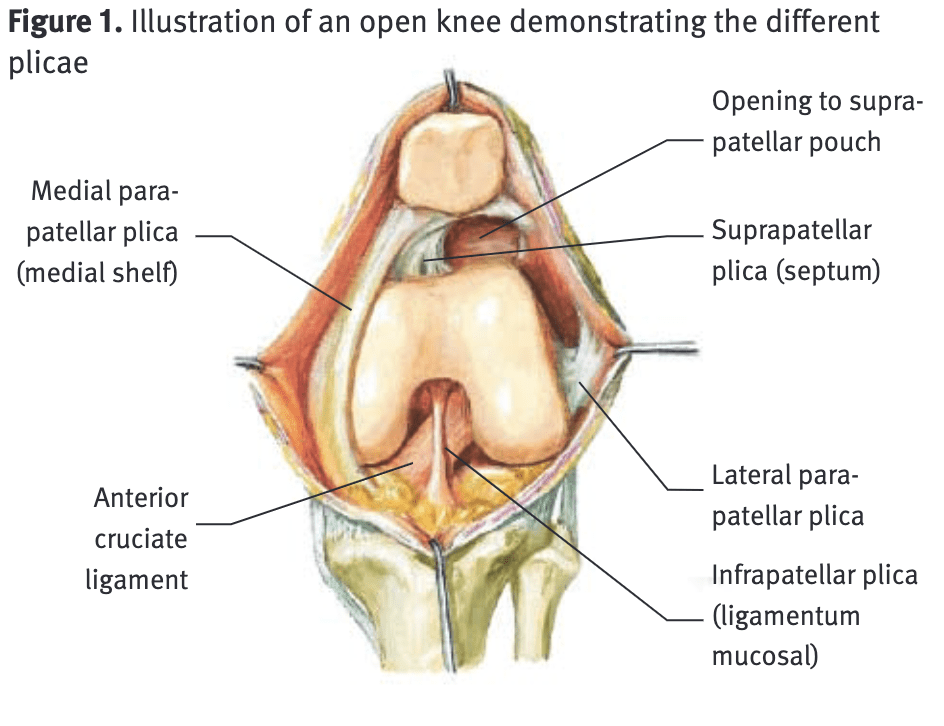
The mediopatellar plica originates in the suprapatellar region and passes inferiorly on the medial aspect of the knee before finding its attachment into the infrapatellar fat pad. I know that’s a ton of jargon, but appreciate the fat pad of your knee has tons of free nerve endings, making synovial plica syndrome extra annoying and irritable.
I warned you that it’s abstract! I leave you with one more metaphor. Picture a plica similarly to the tough, fibrous ridges of a cut bell pepper. They’re pretty similar in overall appearance.
Nothing like a good food metaphor. You’ll never look at bell peppers the same again.
Learn How to Make Knee Rehab A Part of Your Daily Lifestyle
What is synovial plica syndrome?
Plicae become irritable, or “pathological,” when their inherent qualities change due to an inflammatory process. Different things can trigger this inflammatory process including activities that involve repetitive flexion/extension of the knee (think cycling, running, or rowing), direct trauma/blow to the plica, twisting injuries, or increased activity levels. If chronic enough, the plica may become more inelastic, tight, or thickened.
Synovial Plica Syndrome is common in young adults, with the main subjective complaint being an intermittent dull aching pain located in the area medial to the knee cap above the joint line in the supramedial patellar area.
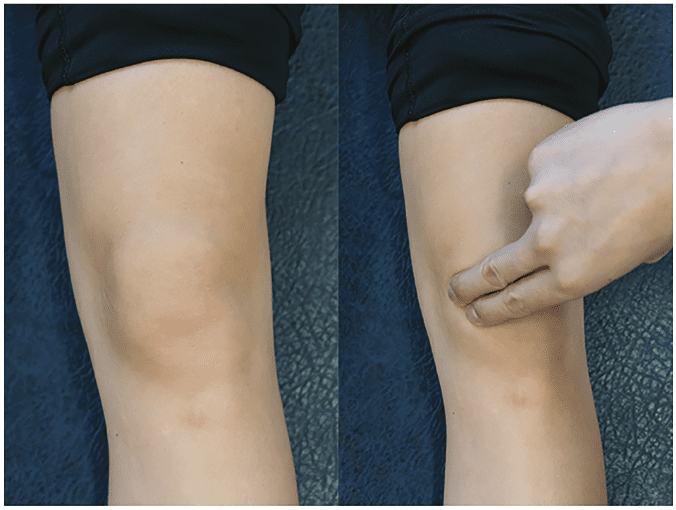
An example of medial knee plica palpation (4).
Other common symptoms that patients report include pain at the front of the knee, snapping sensations along the inside of the knee as the knee is bent, clicking or catching, a “tender band” underneath the skin, knee swelling, pain on squatting, and general stiffness.
Other things that we as clinicians will keep our eye on to ensure aren’t the hidden causes of your pain include meniscal pathology, patellofemoral pain, medial collateral ligament sprain, or osteoarthritis of the medial compartment. True synovial plica syndrome is considered a diagnosis of exclusion, meaning all other possible pathology would be eliminated before narrowing down our focus to the plica. Overall, its incidence is quite low compared to other knee pathologies, typically combing in anywhere from 3.8% to 5.5%.
How can I manage this conservatively?
Almost without question, the initial treatment is going to be conservative in nature. There is typically a very good chance that a well-developed physical therapy program will be enough to improve symptoms. As I always tell my patients, there are very few quick fixes in physical therapy. Please appreciate that you should give a good rehab program 6 to 8 weeks before considering more invasive interventions. Also, appreciate that there are largely no specific, “precision-strike” exercises to do that will directly impact a non-contractile, membranous synovial fold in the capsule of your knee. Rather, there are guiding principles that you can follow, or take to discuss with a musculoskeletal provider of your choice. Some of them are below.
Active Straight Leg Raise With Quad Set
Sample Knee Rehab Program Exercise Video
Lateral Lunge – Slider, Band
Posterior Step Down – RNT

The Prehab membership is the anti-barrier solution to keeping your body healthy. Access state-of-the-art physical therapy, fitness programs, and workouts online in the comforts of your own home or gym! Taking control of your health with exercise & education from the palm of your hand has never been easier. Get access to 50+ programs, 100+ unique workouts, and 3000+ exercises to build your own workout routines. Trial it for free, and learn how to get out of pain, avoid injury, and optimize your health with [P]rehab!
Managing training volume (training load)
Your first step will be taking a step back to look at your training load. Have you recently had a sharp increase in training volume? How about training intensity? Have you recently introduced a new “mode” of exercise (something you haven’t done in the past but recently picked up)? These are all highly individualized questions that we couldn’t possibly begin to dive into the details of in this medium, but they are easy enough to reflect on as an individual or discuss with a clinician or a performance specialist.
READ: UNDERSTANDING TRAINING LOAD

From a conversational perspective, you may need to take a week or two off from your aggravating activity. Find another mode of exercise you can cross-train in to keep up your fitness levels. If there’s a competition date in the future, strategically plan to progressively increase your volume leading up to that date. Depending on that time frame, your progressive loading should be undulating. This means that one day (or week) will increase training volume by a bit, while the next day (or week) will back off a bit to allow some mild recovery. This will progressively repeat, slowing increasing training volume with time, leading up to your competition date. If you’re not an athlete and don’t have an “end date” to work towards, pick a date at 3 to 4 months out from the start date of your rehabilitation. The principles will work the same.
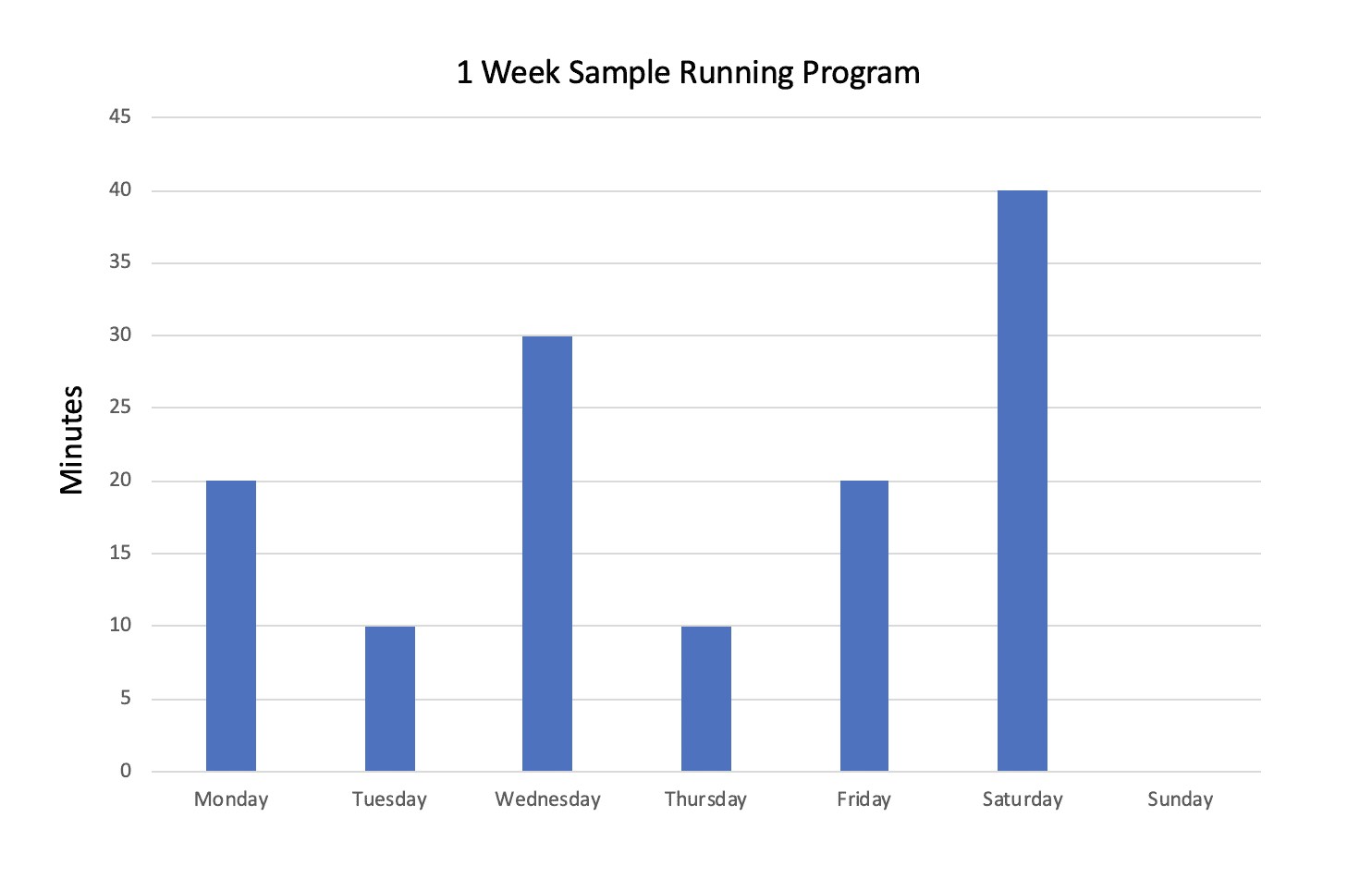
An extremely oversimplified example of undulating load in the form of running minutes. (This doesn’t take into account training intensity or other training variables.)
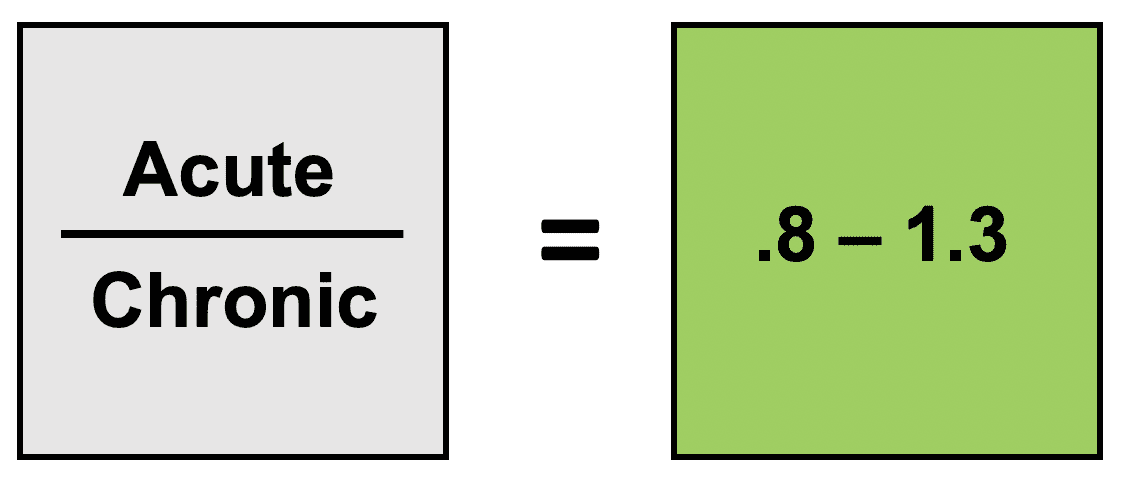
From a clinical or performance perspective, we’d likely look at your acute on chronic workload ratio. This is a ratio coined by a prominent Australian physiotherapist, Tim Gabbett, to monitor training load. Acute training load captures recent training (for example, last week), while chronic training load captures more long-term training (for example, last month).
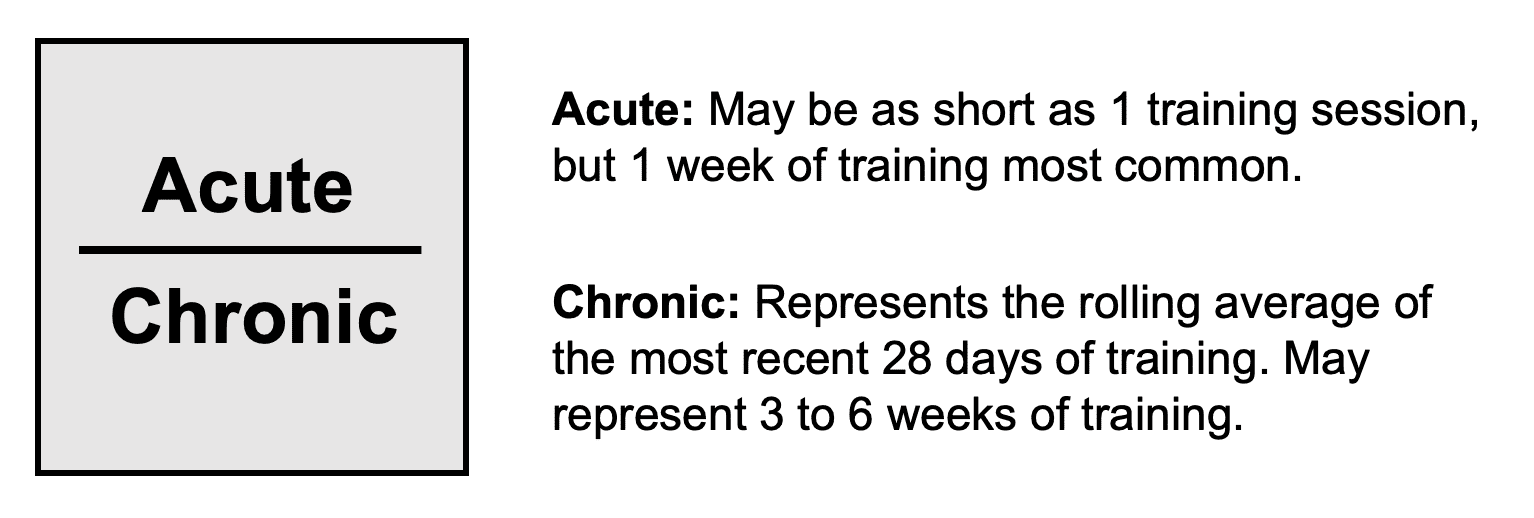
Again, in the case of a runner, add up all the minutes you’ve run (or whatever aggravating activity you’re participating in) in the last week for the acute training load, and then all the minutes you’ve run in the past 28 days for chronic training load. While there is much debate surrounding the most ideal number, Gabbett and researchers have found that an acute-to-chronic ratio of .8 to 1.3 is the most ideal in terms of injury reduction. Being above 1.3 is likely considered “over-training,” while being below .8 is likely considered undertraining. Has a recent spike placed your acute on chronic workload ratio higher than this range?
Therapeutic Exercise Programming (Physical Therapy)
The most successful programs for synovial plica syndrome will include some of the usual overarching themes for knee rehabilitation: improving strength (primarily the quadriceps) and flexibility (quadriceps, hamstrings, and gastroc) of the lower extremity. The trick here will be finding exercises that don’t aggravate symptoms. For a lot of folks with synovial plica syndrome, their symptoms are produced between 30 and 45 degrees of knee flexion.
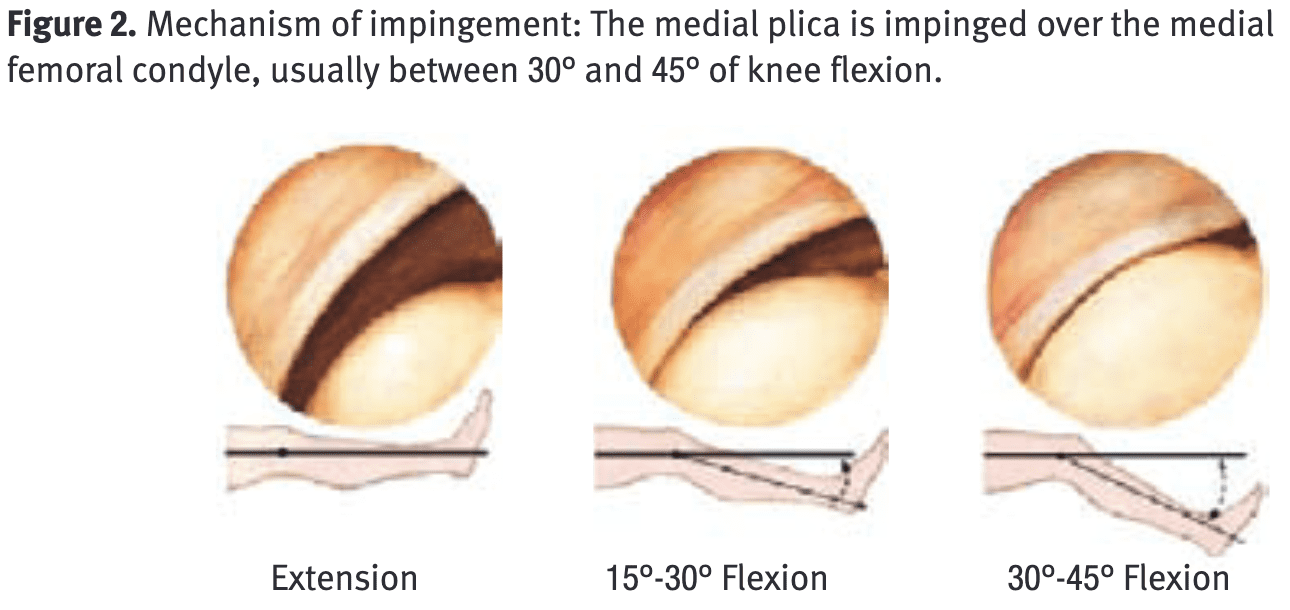
A nice illustration showing impingement of the plica with knee extension (1).
That may mean a seated knee extension machine is a painful choice for you, while a leg press is not. It may mean weighted straight leg raises with blood flood restriction is totally comfortable, but a traditional “short arc quad” is very irritable. It will depend from person to person, and as always, rehabilitation will need to be individualized.
Appreciate that there are so few wrong answers in physical therapy programming, so don’t be afraid to experiment with strength training. Some mild reproduction of symptoms is appropriate (think of any pain that is a “1” or “2” on a scale of “0 to 10”), but anything more is a good indicator to switch to another exercise, decrease load, or alter the range of motion. If you get hooked up with a good physical therapist, he or she can easily help do this for you. If you’re developing your own program, here are some of our favorites in this article.
In a very small study performed between 2002 and 2006, 63 patients with synovial plica syndrome were studied. All of these patients underwent physical therapy programming with the aforementioned pieces of advice (load management, programming focused on improving strength and flexibility of the lower extremity) for 90 days. 55 of these patients improved after conservative treatment, while the remaining 8 opted to undergo arthroscopic surgery.
LISTEN: MAXIMIZING YOUR KNEE REHAB
What other options exist outside of conservative management?
For patients that do not improve with load management and a well-developed physical therapy program, other interventions may be warranted. Getting hooked up with a strong orthopedist or sports fellowship-trained primary care physician will help to decide these next steps. Other interventions may include non-steroidal anti-inflammatories, intra-articular injections or surgical management.
An intra-articular corticosteroid injection can be a useful adjunct in the management of synovial plica syndrome (4), and can often quickly reduce pain levels, allowing a patient to more easily engage in rehabilitation. There isn’t any evidence to use it as a stand-alone intervention (4), meaning neither you nor your physician should consider this an absolute, all-healing quick fix. There will likely be some rehabilitative themes to address regardless. While left up to the preferences of your physician, the injection will likely be 1% lidocaine and typically performed under ultrasound image guidance.
For all remaining patients who continue to struggle, surgical intervention may be warranted. Surgical outcomes are generally reported as good, with some studies suggesting only 10% of patients will continue to have disabling problems (4). For this surgery, an orthopedist will perform an arthroscopic (a minimally invasive surgery performed through several small pin-hole-sized incisions with the guidance of a small camera) excision of the plica, resecting as much of the membranous plical folds that may be responsible for your symptoms. Recovery is typically quick afterward and almost always supplemented with physical therapy.
Some additional food for thought
It’s worth emphasizing again that synovial plica syndrome is a diagnosis of exclusion (meaning it should be the last diagnosis standing after eliminating all other possibilities). In my experience, modern orthopedic surgeons are quick to downplay or scoff at an isolated synovial plica syndrome, better appreciating that your knee pain is likely multi-factorial. He or she (as they should) will maintain a high level of suspicion that another pain generation is at play in the knee, and a full examination and workup will be performed before recommending surgery. Very rarely is an arthroscopic surgery performed to solely excise an irritable plica, and even then, it is often that an orthopedist will begin surgery and find other secondary issues that may actually be the true cause of your pain.
If performed, your orthopedist will make an attempt to completely resect the plica at fault as much as possible. Since the plica is part of the joint lining, it may, unfortunately, grow back if not fully removed (2). In some instances, a scar may develop which can be sensitized and uncomfortable. Naturally, no one wants to make a patient more painful after surgery than they were prior – which speaks to the importance of a detailed workup before deciding on surgery. Again, results are considered good in 75% to 91% of all cases (1), and what I’ve just described is the exception rather than the norm. But again, your situation is individualized, and you should discuss this with your physician and physical therapist. Their advice will always supersede what I can deliver through this medium.
Closing Thoughts
- A plica is a membranous inward fold that is part of the synovial lining of the knee joint capsule. It’s a remaining trace of embryologic knee development.
- Clinically, the mediopatellar plica is the most likely to cause synovial plica syndrome.
- Conservative treatment is the first recommendation, consisting of rest, activity modification, and therapeutic exercise programming.
- There are no specific exercises to recommend for a non-contractile, membranous synovial fold in the capsule of your knee. Rather, there are rehabilitative principles that you will focus on (global strengthening and stretching of the lower extremity).
- For those that still struggle following 6 to 8 weeks of rehabilitation, non-steroidal anti-inflammatories or an intra-articular injection may be recommended by your physician.
- For patients who continue to struggle, arthroscopic surgery may be recommended. Surgical outcomes are typically good. Recovery times are quick should a plica be removed in isolation.
Take control of Your Knee Health!
The knees are true hard-nosed blue-collar workers! They get the job done when the hips and ankles may be taking some extra rest breaks. In this program, you will learn how to restore mobility, learn to get your powerful quadriceps cooperating with you, along with starting the journey to addressing the hip and ankle. In this program, you will learn how to restore mobility, learn to get your powerful quadriceps cooperating with you, along with starting the journey to addressing the hip and ankle.
References
- Sznajderman T, Smorgick Y, Lindner D, Beer Y, Agar G. Medial plica syndrome. Isr Med Assoc J. 2009;11(1):54-57.
- Griffith CJ, LaPrade RF. Medial plica irritation: diagnosis and treatment. Curr Rev Musculoskelet Med. 2008;1(1):53-60.
- Al-Hadithy N, Gikas P, Mahapatra AM, Dowd G. Review article: Plica syndrome of the knee. J Orthop Surg . 2011;19(3):354-358.
- Lee PYF, Nixion A, Chandratreya A, Murray JM. Synovial Plica Syndrome of the Knee: A Commonly Overlooked Cause of Anterior Knee Pain. Surg J (N Y). 2017;3(1):e9-e16.
- Gabbett TJ. The training-injury paradox: Shoulder athletes be training smarter and harder? Br J Sports Med. 2016;50:273-280.
- Camanho GL. Treatment of pathological synovial plicae of the knee. Clinics . 2010;65(3):247-250.
About The Author
Christopher, Lefever, PT, DPT, CSCS, SCS, USAW
[P]rehab Writer & Content Creator
 Originally from Reading, Pennsylvania, Chris graduated with his bachelor’s degree in exercise science and a doctorate of physical therapy from Slippery Rock University. He afterwards completed a sports physical therapy residency at the Memorial Hermann IRONMAN Sports Medicine Institute. He later completed a division 1 sports physical therapy fellowship at Duke University where he worked closely with Duke football, basketball and lacrosse. He returned to Houston afterwards with Memorial Hermann to help develop an emerging division 1 sports physical therapy fellowship.
Originally from Reading, Pennsylvania, Chris graduated with his bachelor’s degree in exercise science and a doctorate of physical therapy from Slippery Rock University. He afterwards completed a sports physical therapy residency at the Memorial Hermann IRONMAN Sports Medicine Institute. He later completed a division 1 sports physical therapy fellowship at Duke University where he worked closely with Duke football, basketball and lacrosse. He returned to Houston afterwards with Memorial Hermann to help develop an emerging division 1 sports physical therapy fellowship.
Present day, he practices with the sports medicine team at the United States Olympic and Paralympic Committee in Colorado Springs, CO. Chris is board certified sports clinical specialist (SCS), certified strength and conditioning specialist (CSCS) and certified in dry needling. He has a particular interest in post-operative rehabilitation of the athletic knee, shoulder, hip and elbow.
Disclaimer – The content here is designed for information & education purposes only and is not intended for medical advice.
About the author : Chris Lefever
Related posts

Latest Blogs

Get Proactive with Prehab
- ✔ Zero wait times, no hidden fees, no barriers to entry!
- ✔ Get out of pain, get stronger, and improve your mobility
- ✔ Access to easy-to-digest physical therapy education videos & resources to learn about your body in the palm of your hand
- ✔ Guidance from trusted Doctors of Physical Therapy






