

Ankle sprains…let’s face it. Most of us have had at least one in our lifetime. When you hear ankle sprain, you envision your foot rolling out when stepping on an uneven surface or missing a step down a flight of stairs. Both of these examples are known as a lateral ankle sprain, which accounts for up to 85-90% of all ankle sprains. These are much more common than other ankle sprains due to the innate mechanism of injury that is more likely to occur in this plane of movement, as well as the weaker soft tissue structures on the outside versus inside of the ankle. However, other ankle sprains do still happen! High ankle sprains are a fairly common injury that is more common in athletics and collision activities. It is important to learn how to rehab a high ankle sprain because it is going to look different than your typical lateral ankle sprain rehab. Follow along as we discuss how to rehab a high ankle sprain!
Prevalence of High Ankle Sprains
High ankle sprains can be a challenging injury to overcome. Sometimes difficult to diagnose accurately, if initially mismanaged, it may lead to chronic issues, including persistent pain, instability, and prolonged recovery. These ankle sprains account for roughly 11-17% of all ankle sprains within the athletic population, and about 10% of all ankle sprains in the general population. These tend to be more common in collision sports, such as lacrosse, rugby, American football, wrestling, and ice hockey. There has been a growing interest in these injuries over the past few years as numbers are trending upwards.
In just 2020 alone, there have been a number of high ankle sprains in the NFL, including All-Pro Players Michael Thomas, Zach Ertz, and Christian McCaffery. These are some of the best athletes in the world, and yes, they are able to overcome these injuries, but this is no walk in the park compared to other injuries. To give you some perspective, these athletes missed about 6-8 weeks of playing time, which is up to one half of the entire regular season! A study by Miller et. al on time to return to play demonstrated that professional football players with high ankle sprains lost significantly more time (2.5 vs. 1.25 weeks), practices (11.7 vs 3.5), and games (1.4 vs 0.3) than those with lateral ankle sprains.
Recover From Your High Ankle Sprain With Our Program!

Have you recently suffered a high ankle sprain and looking for a solution to overcome it? If so, our program is that solution for you! Learn more HERE!
Where At The Ankle Does This Occur?
In contrast to a lateral ankle sprain, high ankle sprains occur higher up the foot, above the ankle joint. The distal tibiofibular syndesmosis is an area of connective tissues that enhances the stability of the talocrural (ankle) joint. Syndesmosis refers to a fibrous joint between two bones that are held together by strong ligaments, with very little to no movement. In contrast to our shoulder for example is extremely mobile, the distal tibiofibular joint is the complete opposite, with very little motion!
This is why when there is an injury to this area of the ankle, it usually requires a high amount of energy, force, and/or trauma.
Ankle Ligaments
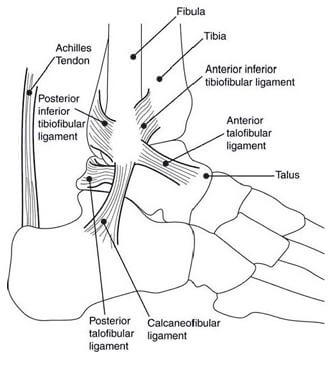
From FootCentre
The primary structures of this joint include the tibia (shin bone), fibula (long bone next to tibia), interosseous membrane, and 4 ligaments: the anterior inferior tibiofibular ligament (AITFL), interosseous ligament, posterior inferior tibiofibular ligament (PITFL), and the transverse tibiofibular ligament. The deltoid ligament, located on the inside of the ankle, is a secondary stabilizer to the distal ankle syndesmosis and may also be injured with a high ankle sprain.
Tibia, Fibula, and Interosseous Ligament
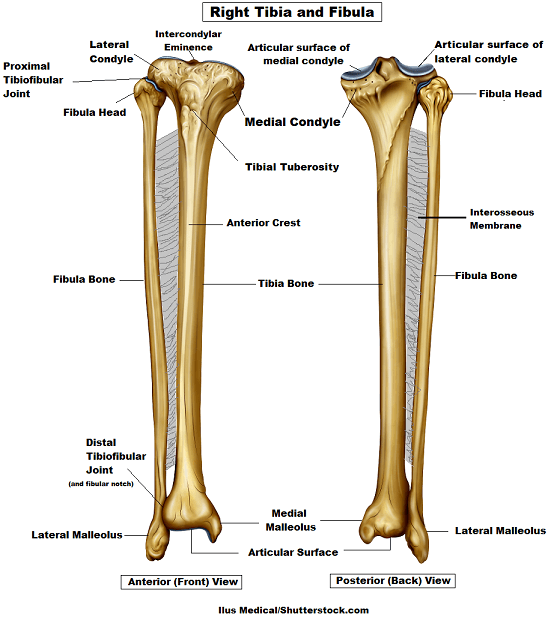 From RegisteredNurseRn
From RegisteredNurseRn
The interosseous membrane is a type of connective tissue that is connected to the tibia and fibula. In some situations, this membrane may become disrupted with more significant high ankle sprains.
Understanding Lateral Versus High Ankle Sprains
Why The Longer Healing Times Than Lateral Ankle Sprains?
So why the longer healing and return to play/function time in comparison to a lateral ankle sprain? There are a couple of reasons. The first being is there usually is a longer, more frequent period of immobilization for high ankle sprains to respect the healing process. However, if someone has a low-grade high ankle sprain, one can start weight-bearing immediately, thus quickening recovery. Moreover, there are often concerns about stability after a high ankle sprain. In some instances, a return to adequate stability for high ankle sprains can take longer, with more rehab time needed.
READ: WHAT YOU NEED TO KNOW ABOUT TISSUE HEALING

High Ankle Sprains: Mechanism of Injury and Risk Factors
Forced External Rotation: Twisting outwards of the ankle is the most common mechanism of injury for a high ankle sprain. What happens during this external rotation motion coupled with a high amount of force is that the talus (ankle bone) causes a separation of the distal tibia and fibula.
In the case of athletics, there are 3 common instances of how this can occur:
- A rapid pivoting motion internally (turning inwards) off of a foot that is planted in an externally rotated position
- When one player applies a valgus force (outwards to inwards force) to another player while the leg is in a planted position
- When there is a direct blow to the outside portion of the heel, which forces the foot and ankle of a fallen or kneeling athlete into external rotation (towards the ground)
High Ankle Sprain Mechanism of Injury

- Forced Ankle Dorsiflexion: There also is a less frequent mechanism of injury for high ankle sprains in which there is a hyperdorsiflexion moment at the ankle. Dorsiflexion of the ankle is when your toes are drawn back towards your shin in the open chain, or when your knee is moving past your toes in the closed chain. Similar to the external rotation mechanism of injury, an excessive amount of dorsiflexion causes the widest portion of the talus to excessively rotate within the ankle mortise. An analogy to conceptualize the separation of the distal tibia and fibula bones is a splitting maul that forces firewood to split apart.
Below are some of the common risk factors for high ankle sprains:
- Wearing rigid boots such as when skiing or playing ice hockey
- Participation in collision sports
- A flat foot
- Previous injury to the foot/ankle complex
- History of ankle instability
Grades of High Ankle Sprains
Depending on the severity of a high ankle sprain, it will dictate prognosis as well as treatment approaches.
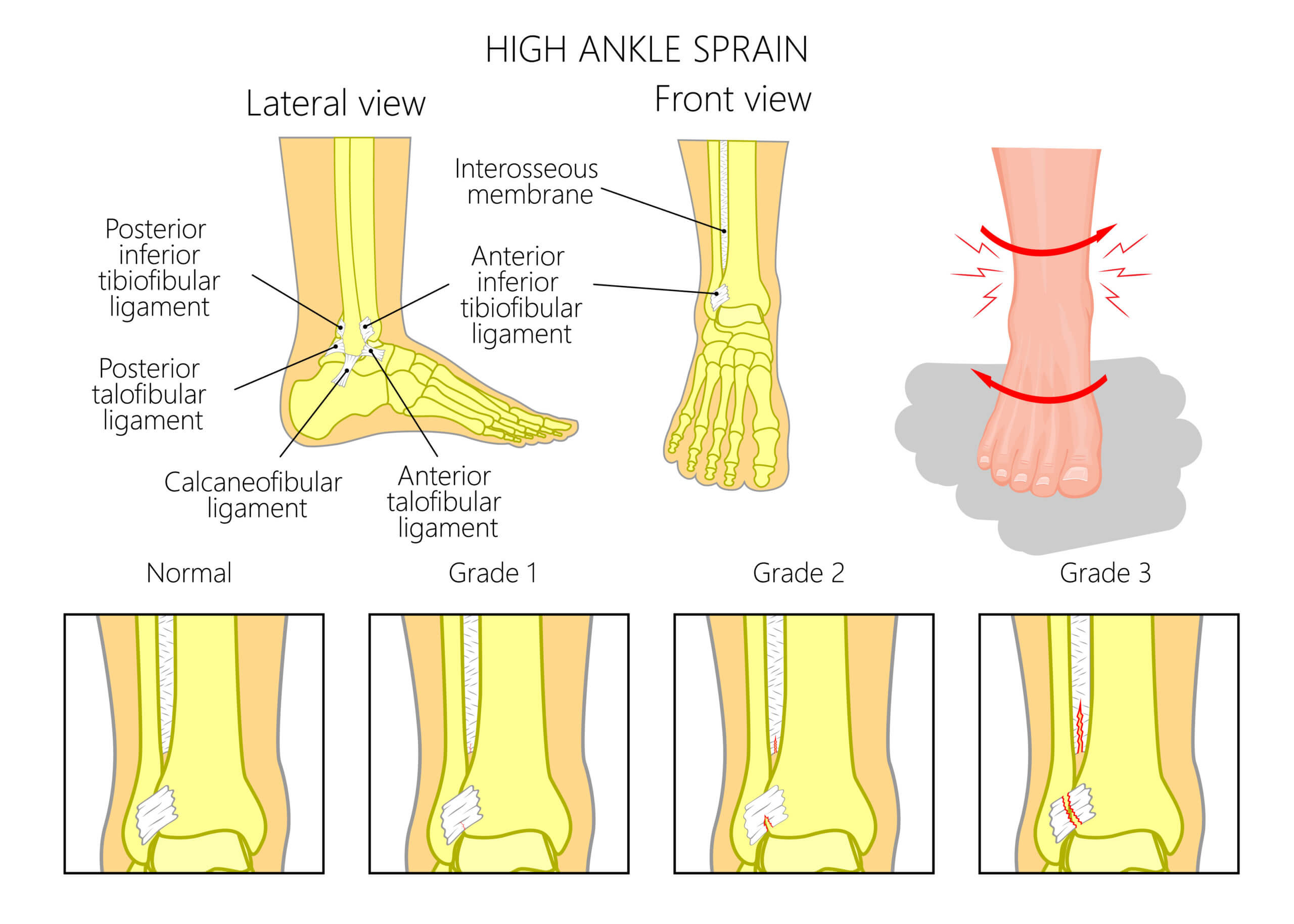
- Grade 1: Involvement of the anterior deltoid ligament and the distal interosseous ligament but without tearing of the more proximal syndesmosis or the deep deltoid ligament. ATIFL usually is tender upon palpation, but due to no diastasis (separation), the injury is stable
- Grade 2: Involvement of the anterior and deep deltoid ligaments as well as a tear in a significant portion of the syndesmosis resulting in an unstable ankle that is still normally aligned on non-stress radiographs.
- Grade 3: Complete disruption of the medial ligaments and severe disruption of the ankle syndesmosis, frequently accompanied by a fracture. These injuries demonstrate a lot of ankle instability.
High Ankle Sprain: The Role of Imaging in Proper Diagnosis
There is a combination of clinical examination tests that can be performed by a practitioner, in addition to specific imaging of the foot/ankle when deemed medically necessary. The American College of Radiology has constructed thorough guidelines for musculoskeletal conditions that allow practitioners to decipher which image may be most appropriate at what time depending on a patient’s clinical presentation.
READ: DO I NEED AN X-RAY AFTER AN ANKLE SPRAIN?

Yes, we usually harp that in many instances, imaging is not required during an initial assessment, you’re are not your MRI readings, etc. However, with a high ankle sprain, this is a situation where initial X-Rays are usually recommended for a couple of reasons:
- To determine if there is any associated fracture if the injury is more severe, as in many instances this is a more intense injury.
- To determine the degree of separation of the distal tibiofibular joint because it is difficult to decipher this with clinical examination.
In regards to imaging, X-Rays specifically, some sprains are easier to detect than others. In an article by Molinari et al, they discussed that incomplete syndesmotic sprains (Grade I or II), X-Rays will still appear normal with no widening of the ankle mortise.
This is why practitioners must cluster together the entire clinical picture, including the mechanism of injury, as well as the signs and symptoms that are discussed next.
High Ankle Sprain Signs and Symptoms
Some of the common signs and symptoms of a high ankle sprain include:
- Difficulty with weight-bearing
- Point tenderness over higher ankle ligaments (ATIFL, PTIFL)
- There also may be tenderness higher up the leg at the interosseous membrane or at the deltoid ligament on the inside of the ankle, depending on the severity of the injury
- Variable edema (swelling) of the foot and ankle
- Swelling is more common higher up the ankle versus lateral ankle sprain which is lower
- If the sprain is more severe such as a tear to the interosseous ligament and/or deltoid ligament, swelling will be more significant, that can be seen on the inside portion of the ankle
- Decreased ability to push off the toes while walking
Learn How To Rehab A Lateral Ankle Sprain
Looking for more content on ankle sprains? Watch our [P]Rehab Youtube Episode on Lateral Ankle Sprains!
So I Have A High Ankle Sprain…Now What?
You now are diagnosed with a high ankle sprain. What happens now? Can I walk? When can I get back on the field? Generally speaking, if someone has a high ankle sprain without significant diastasis (separation) or dynamic instability exemplified on weight-bearing or stress X-rays, that person can be treated non-surgically. Yet in cases of significant instability and associated fractures, surgery will be required.
The Early Phase
- Immobilize and Protect: There usually is a period of immobilization and protection of the injured site. As with any tissue injury, you will want to avoid directions of movement that could strain soft tissue, which is external rotation and excessive dorsiflexion after this injury. There are a variety of orthoses that can be used, such as a walking boot, an ankle stirrup, or a cast in more severe cases.
- Weight Bearing: Difficulty tolerating weight-bearing is a common complaint after this type of injury, which is why relative restrictions are usually indicated in the early phase. The amount of restriction in weight-bearing is based on the severity of the injury and the patient’s symptoms. For instance, if someone had a minor, Grade I high ankle sprain, that individual may be able to tolerate weight bearing right away. However, someone who had a more severe Grade II high ankle sprain might need to be placed in a boot with crutches with a partial weight bearing (PWB) or weight-bearing as tolerated (WBAT) restriction for 1-2 weeks.
- Heel Splints: Sometimes practitioners will want to limit ankle dorsiflexion (toes towards nose motion of the ankle) with a heel splint in the back of a boot for example, but there have been some arguments against this. The rationale to oppose this notion is that the distal tibiofibular joint needs to accept the front portion of the talus (ankle bone) moving into dorsiflexion in order for a normal range of motion to occur. Therefore, if ankle dorsiflexion is strictly prohibited, it can negatively affect the full return in the range of motion.
Because it is common for there to be a period of immobilization after a high ankle sprain, prolonged stiffness of the foot and ankle is common, especially into dorsiflexion. Once you are able to bear weight, restoring dorsiflexion in the closed chain (foot on the ground) is crucial for optimal function. Below we have a podcast dedicated to this topic. We also have an Ankle Dorsiflexion Mobility Overhaul Program that will give you access to a plethora of exercises to optimize your ankle mobility!
LISTEN: THE IMPORTANCE OF ANKLE DORSIFLEXION FOR ANKLE SPRAIN PREVENTION

Early Phase Exercises
As with any other injury, it is important to stay moving in any way that you can to avoid the negative effects of bed rest. The ankle usually has a difficult time combating swelling, but early, open-chain exercises and the method we often praise, POLICE can get you ahead of the game! Here we are showing some ankle and foot exercises, but always remember, you still should train above the injury, such as strengthening in the open chain for the hips. Read our article on how to stay strong after surgery!
Note: An article by Knapik et. al discusses while early range of motion after lateral ankle sprains is commonly prescribed to promote early return to function, early motion after a high ankle sprain may place unwanted stress on the syndesmosis, potentially contributing to heterotopic ossificans formation (abnormal growth of bone) by increasing the zone of secondary injury. This is why there usually is a period of immobilization in a boot before progressing to specific exercises.

The Prehab membership is the anti-barrier solution to keeping your body healthy. Access state-of-the-art physical therapy, fitness programs, and workouts online in the comforts of your own home or gym! Taking control of your health with exercise & education from the palm of your hand has never been easier. Get access to 50+ programs, 100+ unique workouts, and 3000+ exercises to build your own workout routines. Trial it for free, and learn how to get out of pain, avoid injury, and optimize your health with [P]rehab!
Ankle Pumps – Elevated
Sample High Ankle Sprain Rehab Program Exercise
Elevating the foot is great to reduce swelling as it promotes venous return (return of blood back to the heart). Combining that elevation with movement is even better! Ankle pumps not only help push fluid from the area of the foot but also promote an early return in the range of motion. At home, you can use pillows, towels, etc. to prop your foot up.
Standing Weight Shifts
Sample High Ankle Sprain Rehab Program Exercise
Once you are able to begin weight-bearing, get on it!!! Numerous studies have supported safe, early weight-bearing being correlated with improved recovery times and outcomes. You can stand at a kitchen counter at home, or wherever you can place your hands. This is a great drill to practice when first starting to weight bear after an injury so your mind and body can regain this connection of weight-bearing acceptance again before progressing towards more functional, demanding movements.
High Ankle Sprains: Middle Phase
At this point, you have achieved some great milestones. The range of motion is returning, you are able to fully weight bear, the swelling has gone down, and pain is reducing! In this phase, exercise will start to get more progressive at an appropriate rate, with some movements that will continue to load structures surrounding the ankle, further facilitating the healing process. Here are some examples of progressive exercises in this phase.
Y Balance On Foam
Single Leg Balance Anti-Eversion
This is a great exercise to work on after a high ankle sprain for the following reasons:
- It is challenging for the ankle to resist eversion, which is a common mechanism of injury for high ankle sprains. Graded exposure to movements that caused the injury is an important part of the rehab process.
- The incorporation of the resistance band challenges the core. This will provide a foundation to enhance proximal stability which promotes distal mobility!
Late Phase
Time to add on the final touches. If you are returning to sport, it is making sure you can complete all the specific movements optimally. This phase will consist of a return to plyometric movements, cutting, running, and activity-specific re-integration!
Plyometric training is often a missing link between strength training and return to sport for athletes. Read below in our article as we detail plyometric progressions during rehab!
READ: PLYOMETRIC PROGRESSIONS FOR REHAB

Single Leg Squat Catch – BOSU
This is a more advanced proprioception drill that can be implemented in the later stages of rehab. By focusing on catching the ball, Mike is training his hand-eye coordination in addition to proprioception by performing single leg balance on the BOSU.
Lateral Bounding – Band
Bounding is a great way to work on loading the ankle in the frontal plane once sagittal plane movements are becoming easier. Here, Arash has a band around his waist to create a counteracting movement, requiring him to work even harder on his core stabilization and single leg balance!
Closing Thoughts
High ankle sprains are difficult injuries to manage, yet the prognosis is often good! Return to play or full activity can vary depending on the severity of the injury. In a comprehensive review by D’Hooge et. al, the authors discussed that grade I injuries have about a 6-8 week timeline post-injury, but grade III injuries may take 10-14 weeks on average. After a specific injury to the ankle, a differential diagnosis is important to decipher exactly what part of the ankle was injured. Imaging may be a part of the clustering during diagnosis, but paying attention to the history, patient’s presentation, and all other variables is crucial. These injuries are less common than your typical lateral ankle sprain, yet sometimes if more severe, they may take more time to recover from. All in all, put in the work with focused rehab and you will be back to your activities better than ever!
Take Control of Your Ankle Pain Today!

Ankle sprains can be scary and to add fuel to the uncertainty fire there is a lot of misguided information about treating it. We are here to set the record straight because the best treatment is not complete rest, but rather early safe and protected movement. What is done in the initial phases of injury plays a role in the long-term outcome. The goal is that you regain confidence in your ankle’s ability to support movement and generate higher levels of force needed for walking, climbing stairs, and running.
References
- Molinari, A., Stolley, M., & Amendola, A. (2009). High Ankle Sprains (Syndesmotic) In Athletes: Diagnostic Challenges And Review of The Literature. Iowa Orthopedic Journal, 29, 130-138.
- Knapik, D. M., Trem, A., Sheehan, J., Salata, M. J., & Voos, J. E. (2018). Conservative Management for Stable High Ankle Injuries in Professional Football Players. Journal of Sports Health, 10(1), 80-84.
- Miller, B. S., Downie, B. K., & Johnson, P. D. (2012). Time To Return to Play After High Ankle Sprains in Collegiate Football Players: A Prediction Model. Journal of Sports Health, 4(6).
- Hamid N, Loeffler BJ, Braddy W, Kellum JF, Cohen BE, Bosse MJ. Outcome after fixation of ankle fractures with an injury to the syndesmosis: the effect of the syndesmosis screw. J Bone Joint Surg Br. 2009;91(8):1069-73.
- Jelinek JA, Porter DA. Management of unstable ankle fractures and syndesmosis injuries in athletes. Foot Ankle Clin. 2009;14(2):277-298.
About The Author
Sherif Elnaggar, PT, DPT, OCS, SCS
[P]rehab Head of Content
 Sherif graduated from Temple University with a Bachelor’s of Science Degree and a concentration in Kinesiology. He then received his Doctorate of Physical Therapy Degree from DeSales University, graduating with honors of the professional excellence award and research excellence award. After his graduate studies, he served as Chief Resident of the St. Luke’s Orthopedic Physical Therapy Residency Program. Sherif is a Board Certified Orthopedic Clinical Specialist. Sherif focuses on understanding how movement impairments are affecting function while also promoting lifestyle changes in order to prevent recurrences of injury. His early treatment interests include running related injuries, adolescent sports rehab, and ACL rehab in lower extremity athletes. He also has been involved in performance training for youth soccer players. Outside of working as a physical therapist, he enjoys traveling, running and cycling, following Philadelphia sports teams, and spending time with his family.
Sherif graduated from Temple University with a Bachelor’s of Science Degree and a concentration in Kinesiology. He then received his Doctorate of Physical Therapy Degree from DeSales University, graduating with honors of the professional excellence award and research excellence award. After his graduate studies, he served as Chief Resident of the St. Luke’s Orthopedic Physical Therapy Residency Program. Sherif is a Board Certified Orthopedic Clinical Specialist. Sherif focuses on understanding how movement impairments are affecting function while also promoting lifestyle changes in order to prevent recurrences of injury. His early treatment interests include running related injuries, adolescent sports rehab, and ACL rehab in lower extremity athletes. He also has been involved in performance training for youth soccer players. Outside of working as a physical therapist, he enjoys traveling, running and cycling, following Philadelphia sports teams, and spending time with his family.
Disclaimer – The content here is designed for information & education purposes only and is not intended for medical advice.
About the author : Sherif Elnaggar PT, DPT, OCS
Related posts



Latest Blogs

Get Proactive with Prehab
- ✔ Zero wait times, no hidden fees, no barriers to entry!
- ✔ Get out of pain, get stronger, and improve your mobility
- ✔ Access to easy-to-digest physical therapy education videos & resources to learn about your body in the palm of your hand
- ✔ Guidance from trusted Doctors of Physical Therapy








