

Sports performance personnel, sports medicine staff, and athletes of the 21st century have more access to performance metrics than ever before. While this is great news, it presents another problem: what things do we actually care about? And is there any data in specific that can help guide us in injury risk reduction? While more and more research is emerging in the sports medicine world to help us determine this, there are some metrics, present-day, that continue to draw attention from physical therapists and other allied rehabilitative professions. In particular, testing to determine hamstring to quadriceps strength ratios is often performed as part of pre-season fitness assessments in an effort to predict injury risk (anterior cruciate ligament injuries) or as part of post-operative testing batteries to determine when athletes are safe to return to play. But what is a hamstring to quadriceps strength ratio (H:Q ratio)? Does it matter, and should you know yours? Let’s evaluate the thought processes behind the hamstring to quadriceps strength ratio together.
What is a hamstring to quadriceps strength (H:Q) ratio?
So what is a hamstrings to quadriceps strength ratio? (Which we’ll refer to as an “H:Q” strength ratio from here out). Well, it’s essentially what it’s titled: comparing the strength of your hamstring musculature to the strength of your quadriceps musculature. This is done in the form of a ratio, dividing maximal knee flexion strength by maximal knee extension strength (1). These two numbers should be collected at the same knee angular velocity (typical values are 60 degrees per second, 180 degrees per second and 300 degrees per second) (2) and contraction type (isometric, concentric, eccentric). There are several different types of equipment that can be used to collect such data, like an isokinetic dynamometer, or a handheld dynamometer, but we’ll get into that soon. When a H:Q ratio is calculated, it’s often expressed as a ratio like “1:2” or as a percentage like “50%.”

Looking For A Way To Maximize Your Knee Health?

This Knee [P]rehab Program will help you optimize your knee health, working on strength of your quadriceps and hamstrings, as well as incorporating other components of control, stability, mobility, and thoughtful progressions created by Doctors of Physical Therapists and Strength and Conditioning Specialists.
So why does a H:Q ratio matter?
H:Q ratios are thought to be especially influential in the risk reduction of anterior cruciate ligament (ACL) injuries. Non-contact ACL injuries typically occur during intense-high speed actions coupled with quick force productions found during changes of direction while accelerating, decelerating, jumping, or kicking (3). Biomechanically, they are characterized by a combination of motions and rotation at all 3 lower extremity joints including hip adduction and internal rotation, knee valgus, tibial external rotation, tibial anterior translation, and ankle eversion (3). For our purposes today, we’re going to focus on anterior translation.
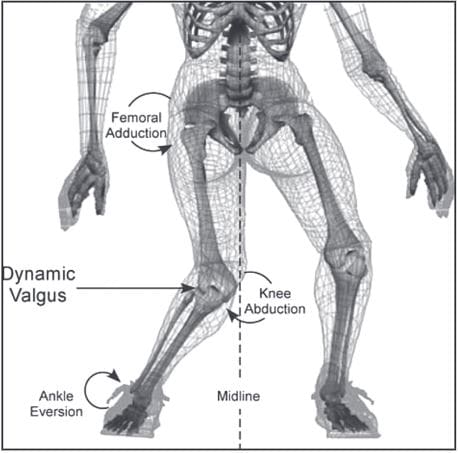
An iconic graphic first published by Hewett, TE, et al in 2005 (4) that illustrates the typical injury mechanism behind ACL tears.
I’d like you to imagine opening your dresser drawer out towards you as you reach in for a pair of socks. This is similar to the anterior translation of the tibia (shin bone) on the femur (thigh bone). Combined with the other aforementioned motions, it contributes to the stresses necessary to rupture an ACL. Now imagine if there were two tethers that held your drawer in place, fighting you as you pulled it out. This, in an oversimplification, is what your hamstrings do to your tibia to prevent anterior translation. They are thought to be protective of your ACL, working to limit the stressors shown in this illustration above. For this reason, knowing the strength of your hamstrings (in relation to your quadriceps) is thought to be a valuable piece of information when determining injury risk for athletes.
READ: HOW TO PREVENT KNEE VALGUS

What is an ideal H:Q strength ratio?
Well, the likely answer is “it depends.” Traditionally, the old adage that most students are taught in physical therapy school is an ideal H:Q ratio is 3:5. In other words, the hamstrings should be 60% as strong as the quadriceps are. This recommendation was originally proposed in 1969 by Klein and Allman (5), and circulates around rehab settings with some accompanying energy as law. Certainly, anything less in an athletic population would be alarming, but in the general public, 60% is likely adequate.
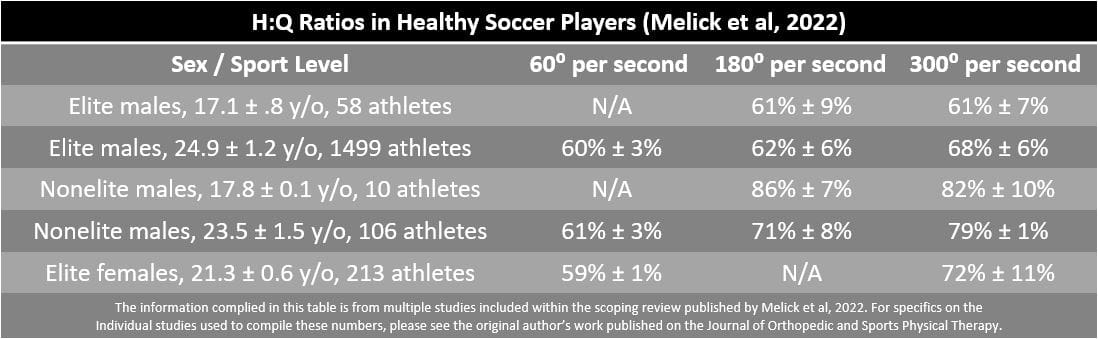
There was a massive scoping review (a synthesis of published literature on a very, very large level) released just this year (6) where researchers looked to broadly define reference values of hamstrings and quadriceps strength metrics. Reference values, or normative values, allow us to compare ourselves to another group much similar to our own demographics (sex, age, sport, etc). Creating reference values is no easy feat and requires a massive amount of athletes to do correctly. Naturally, most literature around the world will examine common sports that researchers have the most access to, meaning soccer, basketball, and handball. Most importantly, these are all common pivoting sports — where most “preventable,” non-contact ACL injuries are most likely to occur.
Researchers quantified information into both “elite” and “non-elite” categories. You may find it helpful to compare your H:Q ratios to some of these published by these researchers (6). See the chart below which outlines H:Q ratios found in healthy soccer players.
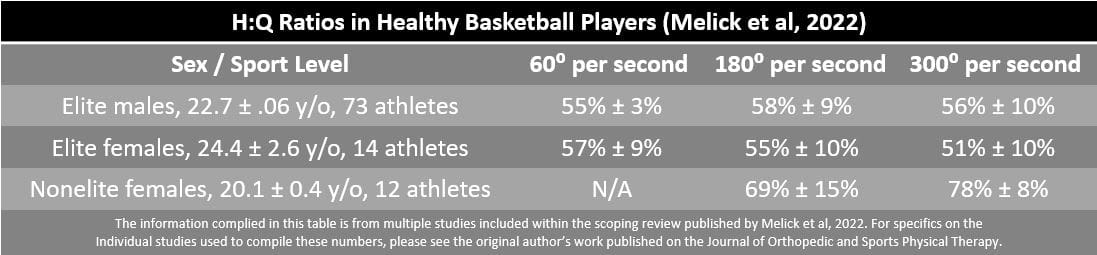
Or, if interested, see the next chart which outlines H:Q ratios found in healthy basketball players.
Well-intentioned, but likely imperfect
Like many standardized rehabilitative measures, having an ideal H: Q ratio does not ensure you’re 100% safe from ACL injuries. A 2021 study out of the Journal of Applied Biomechanics by Bates et al. examined the timing of strain responses in the ACL during simulated landings to create ACL rupture (8). These researchers implanted strain gauges into the ACLs of 35 cadaveric lower extremity specimens and recorded biomechanical data over the course of simulated landing impacts. These researchers determined that non-contact ACL injuries are expected to occur between 0 and 61 milliseconds after initial contact (8), which I’m sure you can appreciate is extremely quick. Of course, this mechanical strain was created largely in part due to anterior tibial translation, which we know is harmful to the ACL when applied in excess. What this study didn’t evaluate is the timing of when the hamstrings typically fire upon landing, leaving a gap in the larger picture. Even if we have an ideal H:Q ratio, is the protective firing of the hamstrings quick enough to blunt the harmful forces of a rough landing? This remains to be undetermined.
The authors of this study were quick to acknowledge their limitations, stating that “muscle contractions would be dynamically changing” in a real-life scenario (compared to the “sterile” laboratory research performed that led to this publication). But interestingly enough, in the simulation used, muscle forces were applied at a constant rate of an H:Q ratio of 1:1 (7), which is a very generous amount of hamstring strength. Remember that as this ratio approaches 100%, the hamstrings have an increased functional capacity for providing stability to the knee (8). Although we lack all of the data to make final conclusions, we can appreciate that strong hamstrings do not guarantee that someone is immune to ACL injuries. As Bates et al. conclude well: “Future work would be desirable to develop an impact model with dynamic muscle force application in a variety of force ratios.”
Even so, from a theoretical or conversational standpoint, the pursuit of improving hamstring strength is certainly sound and is never a bad training goal. It’s theorized that unchecked, highly develop quadriceps musculature contributes to decreased hamstrings coactivation (9), which negatively influences the cascade of biomechanical events that takes place during a non-contact ACL rupture.
How do I collect the data required to determine my H:Q ratio?
I never like to assume, but you’ve likely found this article because you’ve discussed H:Q ratio with your physical therapist, physician, or strength coach already. Often times this ratio becomes a conversational piece, and later a training goal, for many of our patients. Chances are you’ve already performed the testing required to calculate this number, but in the off-chance you haven’t, let’s discuss quickly what equipment you’d need to do so.
Isokinetic Dynamometry
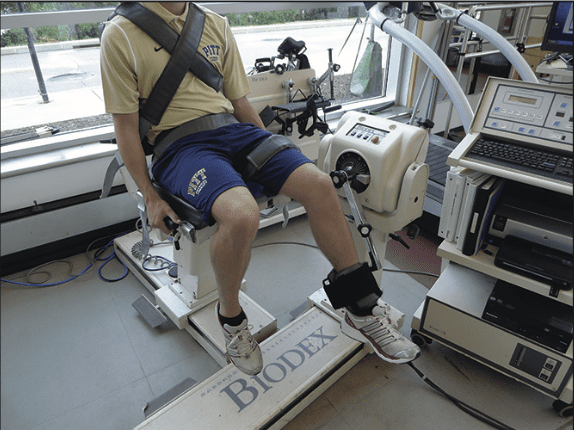
A typical isokinetic dynamometer set-up to test quadriceps and hamstring strength from Sinacore et al, 2017.
Certainly, between the 3 options, we’ll work to discuss, isokinetic dynamometry is the most sophisticated and specialized (and expensive). An isokinetic dynamometer controls the velocity of an exercising limb by means of a preset, integrated variable speed-governing mechanism. As more force is exerted against the lever arm of the isokinetic dynamometer, the energy of the moving limb is absorbed by the apparatus and converted to increased resistance encountered by the limb (10). In other words, movement occurs at a constant predetermined speed.
Almost in entirely all cases, this specialized equipment will be found within well-funded physical therapy clinics or research laboratories. It’s often used to postoperatively test a healing extremity like a knee or shoulder — but can be used across a variety of other joints as well. Performance metrics from this test are typically communicated by the physical therapist to the orthopedic surgeon to illustrate how well someone is doing in their rehabilitation. But of course, its utility can be far greater than this isolated scenario.
If you were to perform this test to determine your H:Q ratio, your physical therapist or clinician would first set you up and individualize the chair and dynamometer settings to your limb length. You’ll get several seat belts to ensure that you don’t compensate with other parts of your body, meaning that the test gets as close to isolating your quadriceps and hamstrings as much as possible. There are a variety of different testing settings that exist, but predominately, most therapists agree upon the following rep and set scheme (6): 5 repetitions at 60 degrees per second, 10 repetitions at 180 degrees per second, and 15 repetitions at 300 degrees per second.
If degrees per second are hard to grasp conceptually, the first set will feel very, very hard. The second set will lighten up a bit, and the third set will be the easiest. You’ll be instructed to complete the test as fast and as hard as you can through a full range of motion. If you have an injured limb, data will be collected on your uninjured side first, then your injured limb second. You’ll get verbal cues from your therapist throughout the test, and if you have any teammates or bystanders around, you can bet they’ll be cheering you on. Completing isokinetic testing is no joke!
Throughout the duration of your testing, the isokinetic dynamometer software will collect a ton of data. Without getting too deep into the weeds, one of the more important metrics is called peak torque. This is the highest output of torque captured during the test from your quadriceps and hamstrings. The software will then take these two peak torques and create your H:Q for you. Again, while the equipment is expensive and the set-up of the machine can look quite cumbersome, isokinetic dynamometry is considered the gold standard for assessing muscle strength (11) in the rehabilitation setting.
*Of note, isometric testing can be performed on an isokinetic dynamometer as well. But for readers who don’t have access to a sophisticated Biodex dynamometer, we’re going to dive into alternative ways to measure isometric strength next.
Isometric Handheld Dynamometry

A typical handheld dynamometer set-up to test quadriceps isometric strength from Sinacore et al, 2017.
In the last decade or so, physical therapy researchers have worked to find other viable options to determine isolated quadriceps and hamstrings strength. As we’ve acknowledged, not everyone has access to an isokinetic dynamometer, so coming up with a reliable alternative was necessary. Thankfully, we have devices called handheld dynamometers, which are relatively cheap and have a huge reach in terms of their utility. They allow us to quantify isometric strength and are most reliable when an external anchor is used to provide resistance (11). Appreciate that in an isometric test the muscle being tested does not change in length; it will feel and look much different than an isokinetic test.
A typical set-up for testing isometric quadriceps strength will look like the photograph listed above, with the athlete seated off the side of a plinth table and a handheld dynamometer fixated to the shin. The knee will be at a 90-degree angle. Typically the clinician will collect data following 3 separate rounds of maximal knee extension efforts lasting 5 seconds each (11).

A typical handheld dynamometer set-up to test hamstring isometric strength from Reurink et al, 2016.
The set-up for testing hamstrings strength will look like the photo shown above with the athlete in prone and the testing leg bent to 90 degrees. The clinician will hold a handheld dynamometer to the shin (12). The testing parameters should stay the same, with 3 separate rounds of maximal knee flexion efforts lasting 5 seconds each. As you can appreciate, testing the hamstring in this fashion doesn’t use an external anchor and relies more on the stability and strength of the clinician, arguably making the measure less reliable. Regardless, the highest isometric strength recordings from these two tests can be used to calculate a H:Q ratio.
A word of caution: although this method of measuring isometric strength is convenient, the results should be interpreted with caution, as there is an increased likelihood for overestimating strength (11) — one of the last things we’d ever want to do when giving an injured athlete permission to return to sport. However, despite this risk, it’s better for a clinician to make decisions based on objective isometric handheld dynamometry data than no data at all.
Looking For A Better Way To Test Muscle Strength? Watch This!
Isometric testing can also be performed with a Tindeq unit as demonstrated by Mike and Adelle. It’s a pretty convenient way to test your strength without the heavy price tag of an isokinetic dynamometer. Check out Mike killing it in the video above!
Isometric Knee Extension and Knee Flexion Machine Testing: 1 Repetition Maximum

A typical knee extension machine set-up to test quadriceps isometric strength (45 degree block) from Sinacore et al, 2017.

A knee flexion machine set-up in a research setting (left leg secured in air to fully isolate right leg) to test hamstring isometric strength from Neeter et al, 2006.
Of the three options we’ve discussed, this equipment is likely the most recognized by the general public: the knee extension and knee flexion machines. While the thought is inherently intuitive for someone interested in calculating a H:Q ratio with this readily available equipment at a typical gym, we don’t recommend it. Researchers have found this method of testing in the quadriceps significantly overestimates function and symmetry (11), even more so than handheld dynamometry. Not to mention, if you’re recovering from an ACL reconstruction, your medical and rehabilitative team may have very specific (and often emotionally charged) thoughts on using the knee extension machine. Many in the field debate its safety on a newly reconstructed ACL (14, 15). Since this is outside the subject matter of this article and not the appropriate place for me to insert my opinions, we don’t recommend performing this on your own without the approval of your orthopedic surgeon and physical therapist. Their detailed and individualized insights supersede the recommendations we can provide through a blog post. However, if you would like to listen to our podcast on this topic, click the link below.
LISTEN: IS THE KNEE EXTENSION MACHINE SAFE TO USE?

All these words of caution explained, if you were to test your 1 repetition maximum on the knee extension machine, researchers have described either testing in 2 ranges of motion: either 90 to 0 degrees of knee flexion (full range) or 90 to 45 degrees of knee flexion (a range prescribed theorized to be safer for a reconstructed ACL). Mechanical stops were used depending on which range was being tested. A successful isometric trial was recorded when a mechanical stop was engaged for 2 seconds at a given weight (11). Please note that participants in this study were given clearance by their surgeon prior to testing. Certainly if looking to determine hamstring isometric strength, the same range and criteria for a successful trial could be prescribed. Technically, a H:Q ratio could be determined from this.
A final word of caution:
Having stronger hamstring musculature is certainly never a bad thing. You’d be hard-pressed to find a clinician or performance coach who’d argue otherwise. But don’t forget the limitations of the H:Q ratio — especially if you’re rehabilitating your knee post-operatively. If injured, chances are your quadriceps strength has dropped significantly. If your hamstrings have either 1.) maintained their strength to some degree or 2.) you’ve focused heavily on hamstring strength and neglected the importance of quadriceps strength, you will see an “artificial” inflation of your H:Q ratio. Taken in isolation, this can make someone feel pretty confident, but in reality, you’ve lowered your strength goals. In other words, never use H:Q ratio as your sole predictor of success. It should be one metric in the long list of return to play measures that should guide decision making between you and your sports medicine team.
Closing Thoughts
- The H:Q metric is often discussed in the sports medicine and performance worlds and certainly valuable to know.
- However, it isn’t fool-proof, meaning even if you have a 1:1 hamstring to quadriceps ratio, it doesn’t ensure you’re immune to injury risk.
- That being said, no one would ever argue against pursuing higher amounts of hamstring strength. It should be a primary goal if rehabbing from an ACL injury, or if completing an ACL injury prevention program.
- If recovering from an ACL reconstruction with a physical therapist, chances are you will have this metric calculated at some point along your rehabilitation. Your orthopedic surgeon may discuss it with you in length and request you improve your H:Q ratio to a certain amount.
- There are several different ways to find your H:Q ratio, ranging in different levels of quality. Isokinetic dynamometry remains the gold standard and isometric handheld dynamometry remains an acceptable alternative. Isometric 1 repetition maximum testing on knee extension and knee flexion machines should be used with a heightened amount of caution and recognized as a last choice, and should require the approval of your physical therapist and orthopedic surgeon.
- As always, objective data should drive decision-making on rehabilitative milestones like a return to running program or return to sport decision; testing with one of the three aforementioned will always be superior to no testing at all.
- The H:Q ratio may be artificially inflated if you have weak quadriceps musculature. This ratio should never be the sole driver of your decision making post-operatively. Rather, include it in the long list of metrics you and your sports medicine team are using to make return to play decisions.
Take Control of Your Knee Health!

Knee discomfort is one of the reasons why people end up sitting out but that’s about to change through the tag team champs of the world: education and movement. The knee must be strong enough to create its own muscular forces and be the traffic director for force passing through. Therefore, to have a successful outcome your program must include not just the knee but the core, hip, and ankle. Teamwork makes the dream work, ready to be part of the team?
References
- Aagaard, P., E. B. Simonsen, S. P. Magnusson, B. Larsson, and P. Dyhre-Poulsen. 1998. “A New Concept for Isokinetic Hamstring: Quadriceps Muscle Strength Ratio.” The American Journal of Sports Medicine 26 (2): 231–37.
- van der Horst N, van Denderen R. Isokinetic hamstring and quadriceps strength interpretation guideline for football (soccer) players within ACL reconstruction: a Delphi consensus study in the Netherlands. Sci Med Footb. In press.
- Hewett, T. E., K. R. Ford, B. J. Hoogenboom, and G. D. Myer. 2010. “Understanding and Preventing ACL Injuries: Current Biomechanical and Epidemiologic Considerations – Update 2010.” International Journal of Sports Physical Therapy 5 (4): 234–51.
- Hewett, T.E., et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am J Sports Med. 2005; 33(4): 492-501.
- Grygorowicz, Monika, Martyna Michałowska, Tomasz Walczak, Adam Owen, Jakub Krzysztof Grabski, Andrzej Pyda, Tomasz Piontek, and Tomasz Kotwicki. 2017. “Discussion about Different Cut-off Values of Conventional Hamstring-to-Quadriceps Ratio Used in Hamstring Injury Prediction among Professional Male Football Players.” PloS One 12 (12): e0188974.
- Melick, Nicky van, Walter van der Weegen, and Nick van der Horst. 2022. “Quadriceps and Hamstrings Strength Reference Values for Athletes With and Without Anterior Cruciate Ligament Reconstruction Who Play Popular Pivoting Sports, Including Soccer, Basketball, and Handball: A Scoping Review.” The Journal of Orthopaedic and Sports Physical Therapy 52 (3): 142–55.
- Bates, Nathaniel A., Nathan D. Schilaty, Ryo Ueno, and Timothy E. Hewett. 2020. “Timing of Strain Response of the ACL and MCL Relative to Impulse Delivery During Simulated Landings Leading up to ACL Failure.” Journal of Applied Biomechanics, April, 1–8.
- Rosene, John M., Tracey D. Fogarty, and Brian L. Mahaffey. 2001. “Isokinetic Hamstrings:Quadriceps Ratios in Intercollegiate Athletes.” Journal of Athletic Training 36 (4): 378–83.
- Baratta, R., M. Solomonow, B. H. Zhou, D. Letson, R. Chuinard, and R. D’Ambrosia. 1988. “Muscular Coactivation: The Role of the Antagonist Musculature in Maintaining Knee Stability.” The American Journal of Sports Medicine 16 (2): 113–22.
- Brown, L.E. (2000). Isokinetics in Human Performance. Human Kinetics.
- Sinacore, J. Anthony, Andrew M. Evans, Brittany N. Lynch, Richard E. Joreitz, James J. Irrgang, and Andrew D. Lynch. 2017. “Diagnostic Accuracy of Handheld Dynamometry and 1-Repetition-Maximum Tests for Identifying Meaningful Quadriceps Strength Asymmetries.” The Journal of Orthopaedic and Sports Physical Therapy 47 (2): 97–107.
- Reurink, Gustaaf, Gert Jan Goudswaard, Maarten H. Moen, Johannes L. Tol, Jan A. N. Verhaar, and Adam Weir. 2016. “Strength Measurements in Acute Hamstring Injuries: Intertester Reliability and Prognostic Value of Handheld Dynamometry.” The Journal of Orthopaedic and Sports Physical Therapy 46 (8): 689–96.
- Neeter, Camille, Alexander Gustavsson, Pia Thomeé, Jesper Augustsson, Roland Thomeé, and Jon Karlsson. 2006. “Development of a Strength Test Battery for Evaluating Leg Muscle Power after Anterior Cruciate Ligament Injury and Reconstruction.” Knee Surgery, Sports Traumatology, Arthroscopy: Official Journal of the ESSKA 14 (6): 571–80.
- Perriman, Alyssa, Edmund Leahy, and Adam Ivan Semciw. 2018. “The Effect of Open- Versus Closed-Kinetic-Chain Exercises on Anterior Tibial Laxity, Strength, and Function Following Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-Analysis.” The Journal of Orthopaedic and Sports Physical Therapy 48 (7): 552–66.
- Noehren, Brian, and Lynn Snyder-Mackler. 2020. “Who’s Afraid of the Big Bad Wolf? Open-Chain Exercises After Anterior Cruciate Ligament Reconstruction.” The Journal of Orthopaedic and Sports Physical Therapy 50 (9): 473–75.
About The Author
Christopher Lefever, PT, DPT, SCS, CSCS, USAW
[P]rehab Writer & Content Creator
 Originally from Reading, Pennsylvania, Chris graduated with his bachelor’s degree in exercise science and a doctorate of physical therapy from Slippery Rock University. He afterwards completed a sports physical therapy residency at the Memorial Hermann IRONMAN Sports Medicine Institute.
Originally from Reading, Pennsylvania, Chris graduated with his bachelor’s degree in exercise science and a doctorate of physical therapy from Slippery Rock University. He afterwards completed a sports physical therapy residency at the Memorial Hermann IRONMAN Sports Medicine Institute.
He later completed a division 1 sports physical therapy fellowship at Duke University where he worked closely with Duke football, basketball and lacrosse. He returned to Houston afterwards with Memorial Hermann to help develop an emerging division 1 sports physical therapy fellowship.
Present day, he practices with the sports medicine team at the United States Olympic and Paralympic Committee in Colorado Springs, CO. Chris is board certified sports clinical specialist (SCS), certified strength and conditioning specialist (CSCS) and certified in dry needling. He has a particular interest in post-operative rehabilitation of the athletic knee, shoulder, hip and elbow.
Disclaimer – The content here is designed for information & education purposes only and is not intended for medical advice.
About the author : Chris Lefever
Related posts



Latest Blogs

Get Proactive with Prehab
- ✔ Zero wait times, no hidden fees, no barriers to entry!
- ✔ Get out of pain, get stronger, and improve your mobility
- ✔ Access to easy-to-digest physical therapy education videos & resources to learn about your body in the palm of your hand
- ✔ Guidance from trusted Doctors of Physical Therapy








