

One complaint that I hear (probably every other month or less) is the claim “my rib is out of place.” Intuitively, I know what my patient is referring to. Ribs, or more accurately the joints in which it shares with the spine or sternum, can get cranky – and damn, they hurt when they do. However, the phrase itself encourages fragility, and from a mechanics standpoint is typically very inaccurate (unless, of course, you’re an emergency medicine physician working up a patient from a high-speed car accident or other high-speed trauma).
So if you’re experiencing rib pain, what can we do about it? What actually causes that pain? Do ribs actually get out place? And are there any specific exercises for rib dysfunction? Let’s dive into the weeds below.
Rib dysfunction is typically self-limiting (goes away on its own) and benign in nature. However, it should be distinguished from other, more serious causes of chest pain (cardiac event) by a medical professional. If in doubt, seek immediate medical attention. The information in this article is not intended to be standalone medical advice.
I work in elite sports as a physical therapist. On a regular weekly basis, I hear our athletes describe pain with terms like “malalignment” and “out of place” more than I’d like to admit. In the grand scheme of the rehabilitative professions, these claims are extremely common and threaded into our culture (whether we as clinicians like it or not). Just about everyone in the general public can conceptualize what these mean on some level, or in many cases, identify with it on a personal basis. Given the frequency, and the publicity, of these pain descriptors, most physical therapists have their “elevator pitch” quickly teed up, ready to help educate their patients to better understand the actual, root causes of their discomfort. Let’s get into the root cause of rib pain, rib anatomy, and exercises for rib dysfunction.
Rib Anatomy 101
The thoracic spine, and the associated ribs that articulate with it, are a unique collection of bony anatomy, complemented by numerous ligamentous (bone to bone), muscular, and neural structures. I imagine if the thoracic spine and ribs were at a house party together, they’d get a lot of attention and free drinks for being pretty cool (in addition to someone probably calling the cops because of dismembered body parts at a party.)
12 thoracic vertebrae stack on top of one another to create your thoracic spine or the mid-portion of your back. The ribs, which make up the thoracic cage that protects your internal organs, include 12 pairs of ribs. These pairs share similarities with their rib neighbors above and below, so they get further categorized into true ribs, false ribs, and floating ribs.
- The true ribs have direct attachments to the sternum (sometimes known as your breastbone) through a unique anatomical connection called the costal cartilage, allowing them to connect directly to the sternum through the sternocostal joint. All in all, these are ribs 1 through 7.
- The false ribs indirectly connect with the sternum, as their costal cartilages connect, ultimately finding their connection through the costal cartilage of the 7th true ribs. The false ribs are considered ribs 8, 9, and 10.
- The floating ribs don’t connect to the sternum and are truly “floating” due to their single attachments to the thoracic spine. These are ribs 11 and 12.
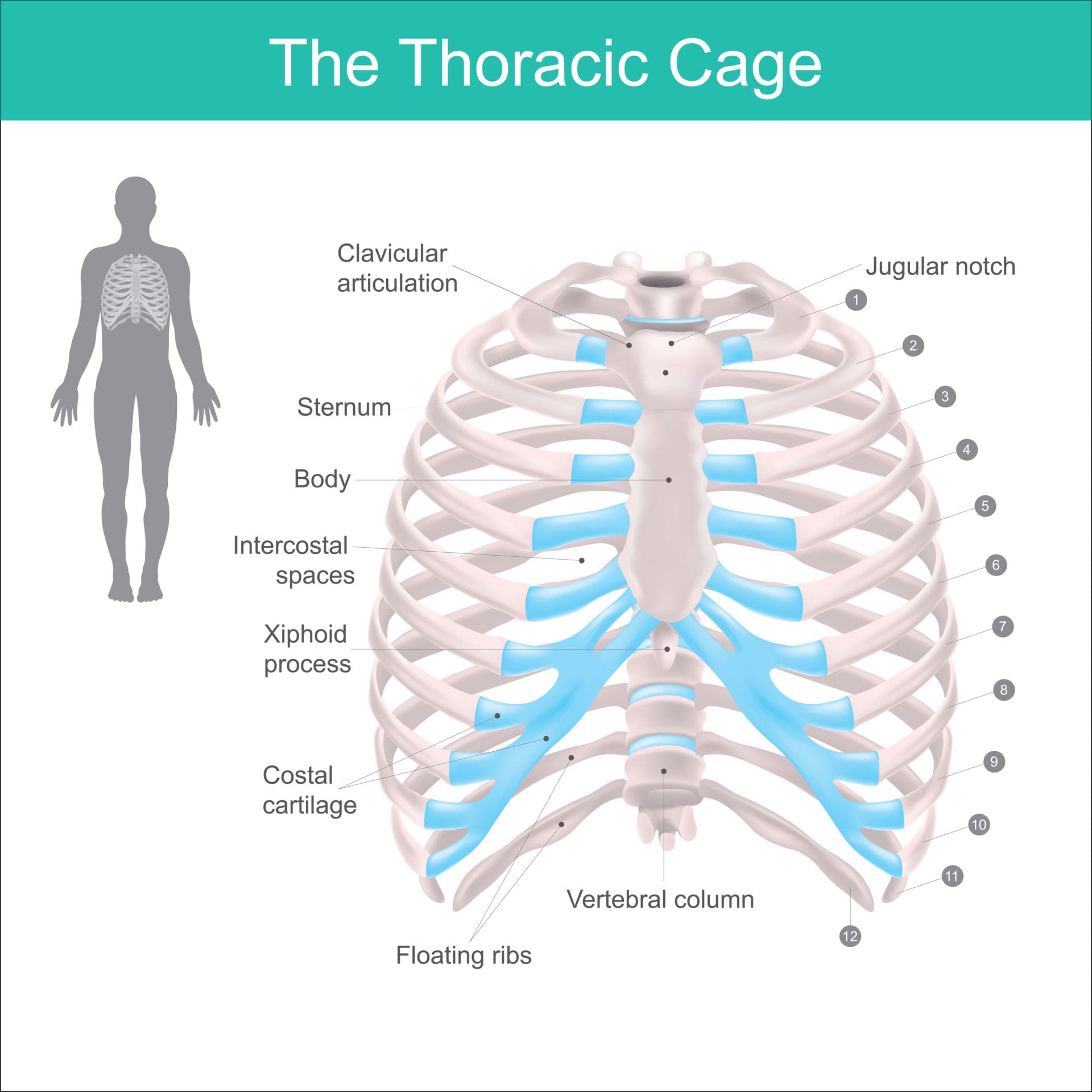
A nice graphic of the ribs and their sternal articulations. Note the blue highlights denote the “costal cartilage,” which is a specialized type of hyaline cartilage that contributes to the elasticity of the walls of the thoracic spine.
Ribs are a Party in the Front, Business in the Back:
So we’ve appreciated the sternal attachments of the true and false ribs in the front, but how about their vertebral attachments in the back? Each rib articulates with two thoracic vertebrae through joints called the costovertebral joints and the costotransverse joint. These joints are richly innervated by collateral branches of the intercostal nerve, remember this in particular, because this will be important later (2).
LEARN MORE ABOUT OUR [P]REHAB THORACIC MOBILITY PROGRAM

Wanting to work on improving the way your ribs function with your thoracic spine? Interested in finding ways to improve your thoracic mobility? Check out our Thoracic Mobility Program designed to do just that! This 8-week program will help you explore the thoracic mobility you have, improve that mobility, and improve that rib health along the way! Get started now!
Taking a step back and thinking of the big picture, appreciate each pair of ribs, their sternal attachments, and their vertebral attachments create a thoracic ring(3). Each thoracic ring consists of 13 joints, making this region of the body a challenging area to make definitive and specific musculoskeletal diagnoses in the presence of pain.
The ribs, their sternal attachments (front), and vertebral attachments (back) create a thoracic ring (3).
The ribs are innervated by the intercostal nerves which supply both sensory and motor branches, coursing between the length of the ribs. Small intercostal muscles exist between the ribs, which assist in breathing, acting to both raise and depress the ribs as the lungs inhale and exhale. And finally, there’s an accompanying artery and vein that run alongside the intercostal nerve as well (1.) Turns out, this is a pretty complicated area of anatomy outside of the usual bony considerations.
That being said, I would be amiss to not mention the thoracic spine and rib cage aren’t entirely exclusive to the musculoskeletal system; they play a role in the respiratory, cardiac, and digestive systems as well. Aside from physical therapists, numerous other providers across multiple medical specialties are often interested in this area of anatomy (3). When a patient develops pain at one of these joints, other causes outside of musculoskeletal pain should carefully be considered as well.
What is a Rib Dysfunction?
In my own humble opinion, the field of physical therapy probably overuses the word “dysfunction.” It isn’t my favorite word, but it is broad enough that it captures a spectrum of symptoms, often packaging and explaining pain in a way that resonates with the patient. It doesn’t inherently plant thoughts of fragility, which many folks fall victim to. After all, it’s scary to be told vertebrae are subluxated (out of place), that your pelvis is rotated, or that a “rib has popped out.” Thankfully, none of these are inherently true (aside from cases of high-speed traumas like a motor vehicle accidents). But they are deeply incorrect and manifest some troubling imagery in the patient’s mind.
The Oxford Dictionary defines dysfunction as an “abnormality or impairment in the function of a specified bodily organ or system.” We can lean into that. And for semantic purposes, we’ll continue to title rib pain as rib dysfunction. We’ll dive into the deeper proposed anatomical explanations behind common bouts of rib dysfunction here soon.
 Learn more about our Thoracic Mobility program through the app as well as dozens of our mid-back and posture-related workouts that can be accessed right at your fingertips!
Learn more about our Thoracic Mobility program through the app as well as dozens of our mid-back and posture-related workouts that can be accessed right at your fingertips!
Explaining Rib Dysfunction & Pain: The Clinician’s Dilemma
When it comes to pain in the spinal column, the thoracic spine is often underserved. Clinicians generally treat it the least of the three spinal segments (cervical, thoracic, and lumbar spine), let alone the unique rib pain and flare-ups that can rise here. Furthermore, the neural complexity of the thoracic spine, along with its many referral patterns, often leads to poor pain source localization (4). And from the clinician’s point of view, lots of other bodily systems refer here including cardiac, renal, pulmonary, and esophageal pain (5). These are real concerns that we don’t want to miss.
Explaining Rib Dysfunction in the Back
As we described earlier, each rib has connections to at least two thoracic vertebrae through the back via the costotransverse and costovertebral joints. These joints are synovial (containing fluid) and surrounded by a joint capsule (ligamentous encasement) which encapsulates the joint itself. This capsule has rich innervation, meaning that it can perceive and communicate detailed information about pain to your nervous system (2).
For whatever reason, these joints may become irritable and hypersensitive. Excessive strain or load, applied to these joints may lead to an abnormal firing of pain receptors in the capsule, often causing local and referred pain (2). The patient, who is seeking some explanation for their pain, can easily grasp the concept that a rib is “out of place” or “subluxated.”
The field of medicine and manual therapy is moving away from this model. I won’t deny it: these false explanations package up the scenario nicely and deliver information to the patient in a way they can understand. But it encourages a vicious cycle.
READ: MASSAGE: WHERE DOES IT FALL IN THE RECOVERY PROCESS?

One of the most significant predictors of a specific injury is a history of that specific injury. Folks with low back pain are more susceptible to developing low back pain. Athletes who rupture their ACL and at far greater risk of doing so again in the future. The same holds for posterior rib dysfunction.
LISTEN: DO YOU NEED SURGERY AFTER AN ACL TEAR?

Imagine someone who has developed sharp posterior rib pain. They seek to consult with a medical provider that informs them a “rib has come out of place.” That provider may treat with a manipulation (“pop” the joint with a hands-on technique), and the patient experiences an immediate reduction in symptoms. While I’m fine with this as an initial intervention, the narrative encourages fragility and removes control from the patient to self-manage. And sure enough, the pattern will repeat in the future should (or when) that patient will likely experience similar rib pain again.
As a whole, appreciate that posterior rib pain is likely due to an irritable joint capsule surrounding facet joints that connect the rib to your thoracic spine. I prefer to call these joints “cranky,” “irritable” or a “hot spot.” While these are a tad generic, and admittedly don’t sound nearly as cool as outdated biomechanical nomenclature (subluxation), they are far less threatening and have a softer impact on the patient’s perception.
Explaining Rib Dysfunction in the Front
Rib pain can also present anteriorly as well (where the ribs insert into the sternum). Pain is most commonly localized to one side of the sternum, somewhere between the second through the fifth costochondral junction (6). Oftentimes, more than one junction is affected (6). It’s usually self-limiting in nature, meaning that it will often resolve on its own. Frustrating enough, we don’t fully understand what even causes it, but its onset is usually associated with repetitive activities with the upper extremities or deep breathing (7). Rib pain of this nature is typically called costochondritis. Anecdotally, I’ve seen it commonly in swimmers, especially when coming off a long break or the off-season.
For completeness, Tietze Syndrome is a close cousin to costochondritis. The two are often used interchangeably but are different in presentation. Tietze Syndrome is a rarer disorder that typically involves the swelling of a single costal cartilage, usually the second rib (6). In comparison, costochondritis typically does not involve swelling.
EARN MORE ABOUT OUR [P]REHAB THORACIC MOBILITY PROGRAM

Non-Musculoskeletal Referrals (Red Flags)
Any article on rib pain would be amiss to not pay homage to potential “red flag” referral sources that may warrant quick referral to our physician partners. In a study of costochondritis in an emergency department, 6% of patients with pain reproduced by palpation over the costochondral joints (thought to have chest pain due to costochondritis) were also diagnosed with a myocardial infarction (8). In another emergency department study of noncardiac chest pain, almost 3% of patients had adverse coronary events by a 30-day follow-up (9).
The American Academy of Family Physicians recommends that patients suspected of having costochondritis who are older than 35 or who display symptoms, signs, or history of coronary artery disease, infection, or other serious conditions get further work-up including a chest x-ray and electrocardiography (6). Certainly, any anterior chest pain that presents with shortness of breath, jaw pain, or left shoulder pain should be evaluated by a physician for cardiac-related issues (5).
Other red flags to be aware of include weight loss, night sweats, increased pain at night, or pain not affected by positional changes. All of these questions will be asked by a clinician should you seek formal treatment. When in doubt, seek to consult with your physician.
Treating Rib Dysfunction in the Front (Costochondritis)
Costochondritis is a tricky problem to manage. Unfortunately, there are no “slam-dunk” rehabilitative interventions. As we’ve mentioned before, it’s usually self-limiting in nature, and typically resolves within weeks (6). In severe cases, it may extend into months. From a medical standpoint, it’s usually managed with pain relief through acetaminophen, nonsteroidal anti-inflammatories, or other analgesics (6). Consult with your physician on this for specifics.
From a rehabilitative standpoint, activity modification will be hugely beneficial here. If there’s a precipitating activity that was believed to have contributed to the flare-up, this should be limited or avoided for a short duration. For example, if you’ve recently been practicing a ton of breaststroke in the water, it would be wise to switch to some stationary biking. You’ll want to minimize the load and stress applied to your sternum and costal cartilage.
Certain exercises in the gym to avoid during the height of a costochondritis exacerbation include any type of pectoral / chest flies (machine or dumbbells), traditional bench press, or push-ups. All three of these will stretch the anterior chest under load and likely prolong symptoms.
Gentle movement and mobility exercises may prove beneficial here, but putting the costal cartilage under aggressive and repetitive tension won’t help speed up the condition acutely. Instead, some light stretching with mild symptoms is likely appropriate. The intent here is not to push deep into end ranges. There are very few pieces of scholarly rehab-based literature that exist on the topic, but two papers suggest that light mobility drills provide meaningful improvements for patients(7,10). However, in my opinion, that time and activity modification likely are the two biggest drivers in symptom resolution, working through what feels comfortable with exercises for rib dysfunction.
The above exercise is a good way to work on introducing some healthy mobility through the posterior and anterior mid-back region. As I mentioned, explore ranges that feel comfortable with the onset of only mild symptoms.
Treating Posterior Rib Dysfunction (Costovertebral or Costotransverse Joint Irritation)
From a rehabilitative standpoint alone, there are several different routes to pursue if you’ve developed some costovertebral or costotransverse rib. If you have access to a physical therapist or chiropractor, a simple manipulation of the joint believed to be responsible usually provides some immediate, albeit sometimes short-duration, relief (11,12). We don’t fully understand the mechanisms behind why these techniques work, but generally, physical therapists agree that a manipulation brings some potent movement and neurological input to a joint that’s not moving well or irritable.
READ: IS CRACKING JOINTS BAD? THE SCIENCE OF JOINT CAVITATIONS

The “pop” you’ll hear isn’t anything being aligned, rather, it’s air being released from a joint. 13,14 Typically this intervention should help movements involving the hypomobile joint feel less irritable afterward, providing a valuable window for movement. And as a disclaimer, you don’t need an audible “pop” to reap the benefits of manipulation (15).
In terms of exercise, there isn’t one specific type or intervention that we’d recommend. Instead, we’ll focus on some basic principles.
First, explore your symptoms. We recommend performing an abbreviated movement examination (video above). This includes thoracic flexion, extension, side bending left, side bending right, rotating left, and rotating right. You’ll likely find some movements feel better, while others provoke your symptoms. Find the movement that either reduces or resolves , your rib discomfort – this is called a directional preference. Whatever this direction maybe will ultimately drive your therapeutic exercise programming acutely. You should perform this multiple times throughout the day, working to improve the range of motion intentionally as tolerance improves further (16,17). Some examples of exercises for rib dysfunction that you can use to explore your preferred motion can be found below:
Explore thoracic extension with the above exercise, flexion with the exercise below, and rotation with the last exercise. Take note of how your symptoms feel and which movements seem to feel better as compared to others.
These are principles generally threaded into common day exercise prescriptions for spine pain (especially the lumbar and cervical spine) that are the work of Robin McKenzie, a famous New Zealand physical therapist (1931-2013) and pioneer in the field of musculoskeletal rehabilitation.
As time passes, re-test other movements that were previously aggravating. You should find with time that they diminish in severity and that you’ll gain motion and tolerance here. Explore these directions of movement more, pushing enough only to mild levels of discomfort. Generally, we’d recommend pushing no further than a “3” out of “10” on a pain scale of 0 to 10. While exploring other planes of movement, continue your primary efforts into the directional preference you’ve already identified. With these principles and time, you should be able to effectively self-manage your rib discomfort to the point of a successful outcome.
Summary
- The ribs are categorized into true (ribs 1-7), false (8-10), and floating ribs (11-12).
- The ribs (except the false ribs) connect anteriorly to the sternum via the costal cartilage and connect posteriorly to the thoracic vertebrae through the costovertebral and costotransverse joints.
- While there are several different mechanisms behind rib pain, typically anterior rib pain is the result of developing costochondritis or Tietze’s Syndrome. Posterior rib pain is typically the result of an irritable costovertebral or costotransverse joint.
- costochondritis is usually managed with activity modification, over-the-counter pain relief, and light mobility drills. It typically resolves on its own with time.
- An irritable costovertebral or costotransverse joint generally responds well to manipulation by a licensed clinician acutely. Thoracic mobility drills prescribed in the directional preference of the patient are typically the general first line of exercise programming. These will also resolve with time.
- Unless you’ve recently been involved in a high-speed trauma like a car accident, your rib is not out of place. This explanation of pain is outdated, provides a false narrative, and removes control from the patient to self-manage their symptoms.
- Lots of different bodily systems (cardiac, respiratory, and digestive systems) can refer to the anterior chest wall. When in doubt, consult with your physician – especially if shortness of breath, jaw pain, or left shoulder pain5 is additionally present.
References
- Safarini OA, Bordoni B. Anatomy, thorax, ribs. StatPearls, NCBI Bookshelf. Published July 11, 2022. Accessed January 21, 2023. https://www.ncbi.nlm.nih.gov/books/NBK538328/
- Arroyo JF, Jolliet P, Junod AF. Costovertebral joint dysfunction: another misdiagnosed cause of atypical chest pain. Postgrad Med J. 1992;68(802):655-659.
- Lee DG. Biomechanics of the thorax – research evidence and clinical expertise. J Man Manip Ther. 2015;23(3):128-138.
- Young BA, Gill HE, Wainner RS, Flynn TW. Thoracic costotransverse joint pain patterns: a study in normal volunteers. BMC Musculoskelet Disord. 2008;9:140.
- Fruth SJ. Differential diagnosis and treatment in a patient with posterior upper thoracic pain. Phys Ther. 2006;86(2):254-268.
- Proulx AM, Zryd TW. Costochondritis: Diagnosis and Treatment. American Family Physician. 2009;80(6):617-619.
- Zaruba RA, Wilson E. Impairment based examination and treatment of costochondritis: A case series. International Journal of Sports Physical Therapy. 2017;12(3):458-467.
- Disla E, Rhim HR, Reddy A, Karten I, Taranta A. Costochondritis. A prospective analysis in an emergency department setting. Arch Intern Med. 1994;154(21):2466-2469.
- Miller CD, Lindsell CJ, Khandelwal S, et al. Is the initial diagnostic impression of “noncardiac chest pain” adequate to exclude cardiac disease? Ann Emerg Med. 2004;44(6):565-574.
- Rovetta G, Sessarego P, Monteforte P. Stretching exercises for costochondritis pain. G Ital Med Lav Ergon. 2009;31(2):169-171.
- Kelley JL, Whitney SL. The use of nonthrust manipulation in an adolescent for the treatment of thoracic pain and rib dysfunction: a case report. J Orthop Sports Phys Ther. 2006;36(11):887-892.
- Schiller L. Effectiveness of spinal manipulative therapy in the treatment of mechanical thoracic spine pain: a pilot randomized clinical trial. J Manipulative Physiol Ther. 2001;24(6):394-401.
- Evans DW, Breen AC. A biomechanical model for mechanically efficient cavitation production during spinal manipulation: prethrust position and the neutral zone. J Manipulative Physiol Ther. 2006;29(1):72-82.
- Unsworth A, Dowson D, Wright V. “Cracking joints”. A bioengineering study of cavitation in the metacarpophalangeal joint. Ann Rheum Dis. 1971;30(4):348-358.
- Flynn TW, Fritz JM, Wainner RS, Whitman JM. The audible pop is not necessary for successful spinal high-velocity thrust manipulation in individuals with low back pain. Arch Phys Med Rehabil. 2003;84(7):1057-1060.
- Kjellman G, Oberg B. A randomized clinical trial comparing general exercise, McKenzie treatment and a control group in patients with neck pain. J Rehabil Med. 2002;34:183-190.
- Clare HA, Adams R, Maher CG. A systematic review of efficacy of McKenzie therapy for spinal pain. Aust J Physiother. 2004;50(4):209-216.
About The Author
Christopher Lefever, PT, DPT, SCS, CSCS, USAW
[P]Rehab Writer & Content Creator
 Originally from Reading, Pennsylvania, Chris graduated with his bachelor’s degree in exercise science and a doctorate of physical therapy from Slippery Rock University. He afterward completed a sports physical therapy residency at the Memorial Hermann IRONMAN Sports Medicine Institute. He later completed a division 1 sports physical therapy fellowship at Duke University where he worked closely with Duke football, basketball, and lacrosse. He returned to Houston afterward with Memorial Hermann to help develop an emerging division 1 sports physical therapy fellowship. Present day, he practices with the sports medicine team at the United States Olympic and Paralympic Committee in Colorado Springs, CO. Chris is a board-certified sports clinical specialist (SCS), certified strength and conditioning specialist (CSCS) and certified in dry needling. He has a particular interest in post-operative rehabilitation of the athletic knee, shoulder, hip, and elbow.
Originally from Reading, Pennsylvania, Chris graduated with his bachelor’s degree in exercise science and a doctorate of physical therapy from Slippery Rock University. He afterward completed a sports physical therapy residency at the Memorial Hermann IRONMAN Sports Medicine Institute. He later completed a division 1 sports physical therapy fellowship at Duke University where he worked closely with Duke football, basketball, and lacrosse. He returned to Houston afterward with Memorial Hermann to help develop an emerging division 1 sports physical therapy fellowship. Present day, he practices with the sports medicine team at the United States Olympic and Paralympic Committee in Colorado Springs, CO. Chris is a board-certified sports clinical specialist (SCS), certified strength and conditioning specialist (CSCS) and certified in dry needling. He has a particular interest in post-operative rehabilitation of the athletic knee, shoulder, hip, and elbow.
Disclaimer – The content here is designed for information & education purposes only and is not intended for medical advice.
About the author : Chris Lefever
Related posts



Latest Blogs

Get Proactive with Prehab
- ✔ Zero wait times, no hidden fees, no barriers to entry!
- ✔ Get out of pain, get stronger, and improve your mobility
- ✔ Access to easy-to-digest physical therapy education videos & resources to learn about your body in the palm of your hand
- ✔ Guidance from trusted Doctors of Physical Therapy








