

The biceps is a very important muscle in our upper arm that plays an integral role in our function. The muscle runs from the front of the shoulder to the elbow. It has two proximal tendon attachments to the shoulder and one insertion point at the elbow. The function of the biceps is to flex the elbow and to supinate, or rotate, the forearm into a palm up position. It also assists in shoulder flexion, helping to raise the arm forward. One of these two tendons rarely suffers from injury while the other tendon is particularly susceptible to pain, injury and associated shoulder dysfunction! In this article, you’ll learn why that is, as well as the risk factors, treatment, and prevention strategies to take care of that pesky biceps pain. Follow along in this article as we demonstrate some awesome biceps tendon pain exercises!
Biceps Structure and Function
The biceps muscle has two proximal tendinous attachment points. These are known as the long and short heads of the biceps. The short head tendon runs medially relative to the long head and attaches to the coracoid process of the scapula. The long head of the biceps attaches to the supraglenoid tubercle of the scapula along with the superior labrum. The long head tendon passes through the subacromial space and is held in place as it exits the shoulder by the bicipital groove, the coracohumeral ligament, and the superior glenohumeral ligament, and the subscapularis and supraspinatus tendons.
The borders of the subacromial space are defined by the head of the humerus, the acromion, coracoacromial ligament, and the acromioclavicular joint. In addition to the long head tendon of the biceps, this space also includes the rotator cuff tendons and the subacromial bursa. This pathway of the long head tendon contributes to the high injury rate and pain associated with it, relative to the short head, whose pathway down the arm has little to no chance of getting impinged or disrupted.
Shoulder Anatomy
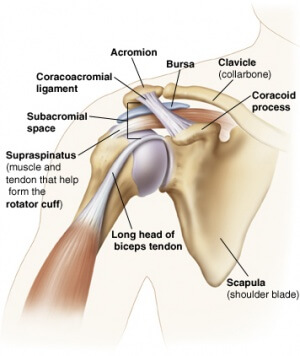
From Physiopedia
Risk Factors for Proximal Biceps Injury
The following are factors that can increase your chances of suffering from biceps tendon pain and injury.
- Age: With increasing age, tendons become stiffer and less elastic and there is also a reduction in blood supply, all of which puts an individual at greater risk for tendinous injuries.
- Overhead activities and overuse: Repetitive and excessive or forceful shoulder activities can place the shoulder at risk for biceps wear and tear through tension, compression or shearing forces.
- This is especially common in throwing athletes, with what is known as the ‘peel back mechanism’. The more one throws with higher amounts of volume, and/or the shoulder joint is not as strong or mobile as it should be, the biceps tendon can begin to pull on the labrum of the shoulder, resulting in an overuse injury. The ‘peel back mechanism’ is best visualized as trying to pull a weed out of the ground – you pull up and in different directions to yank it out!
- Corticosteroid and anabolic steroid use: Injections or oral ingestion of corticosteroids as well as anabolic steroids can increase one’s risk for tendon rupture.
- Smoking: Smoking impairs blood supply throughout the body which can delay tendon healing. Research shows that smoking is associated with tendinopathy and persistent shoulder pain. Smokers are at a 7.5x greater risk of biceps rupture of the distal tendon compared to their non-smoking counterparts (1).
Are You Dealing With Biceps Tendon Related Shoulder Pain?

The Shoulder [P]Rehab Program is a physical therapist developed, step-by-step program that teaches you how to optimize your shoulder health. This 4-phase program will expose you to various scapula and shoulder strengthening and stabilization exercises supported by science. This program will bulletproof your shoulders for anything life throws at you! Learn more HERE!
Common Biceps Injuries
Biceps Tendinitis begins with inflammation and tenosynovitis, or swelling of the tendon sheath. Onset is usually secondary to overuse and repetitive micro traumas. It most commonly affects the proximal, long head biceps tendon. As previously stated, this tendon is particularly susceptible to impingement as it runs through a tight space along the anterior shoulder known as the bicipital groove and travels up along the anterior aspect through the subacromial space. The inflammation can lead to an increase in the size of the tendon, causing further irritation within the already limited space.
Biceps tendinitis is common in overhead and contact athletes, such as baseball and softball, volleyball, as well as gymnastics, swimming and martial arts. The majority of biceps tendinitis cases are seen in conjunction with other shoulder injuries, including rotator cuff pathology, glenohumeral internal rotation deficit (GIRD), superior labral tears, and subacromial impingement. Other contributing factors that predispose individuals to biceps tendinitis include scapular dyskinesia, ligamentous instability, and anterior capsular laxity or posterior capsule tightness, as well as weak or poor core control.
Proximal biceps tendonitis can worsen and become tendinosis as the tendon undergoes thickening of the sheath, along with fibrotic changes and reduced vascularity to the region. Mobility of the tendon reduces with degeneration, scarring, and adhesions. Impaired tendon mobility further exacerbates the shearing forces along the length of the tendon as it passes across the shoulder. The tendon itself can rupture near the bicipital groove or at the proximal attachment point along the superior glenoid tubercle.
READ: TENDINITIS VERSUS TENDINOSIS

Biceps tendon tears. Partial or full tears of the proximal tendon of the biceps long head are much more common than tears of the short head tendon. Biceps tendon ruptures are often due to overuse activities seen in sports and certain job duties, or due to acute injury. Overuse injuries occur gradually over time with the biceps tendon fraying due to repetitive shoulder motions. Acute injuries such as a fall can also cause a rupture of the tendon. As with biceps tendinitis, activities that require overhead movements such as swimming, tennis, and baseball increase one’s risk of biceps tear.
For acute injuries, there is often an immediate, sharp pain at the shoulder along with a popping or snapping sound. Bruising along the shoulder down to the elbow may occur within the next few days as well. Other symptoms include weakness and difficulty with elbow motion and rotating one’s palm up, known as supination, along with pain along the upper arm. With full thickness tears, the biceps muscle can descend, creating a bulge near the elbow, known as Popeye’s sign, as the tendon is no longer able to suspend it in place.
Biceps Tendon Rupture – Popeye Deformity

One of the benefits of having two proximal tendon attachments for the biceps is that individuals with full tears of the proximal long head biceps tendon can often regain full or nearly full strength and range of motion due to the muscle action of the biceps tendon short head!
SLAP tears. SLAP stands for Superior Labrum Anterior and Posterior. A SLAP tear refers to a tear of the shoulder labrum along the superior or top portion and the tear runs from anterior to posterior. If you think of the shoulder joint and labrum like the face of a clock, the tear would run roughly from 10:00 to 2:00 (it may be bigger or smaller, depending on the extent of the tear). This tear impacts the proximal long head of the biceps tendon due to the tendon’s attachment point on the superior labrum. SLAP tears commonly elicit shoulder pain, weakness, and loss of some shoulder functioning.
Biceps Tendon Instability. Instability of the proximal tendon of the biceps long head can lead to dislocation or subluxation of the tendon out of the bicipital groove. This can occur with overuse and repetitive wearing, or with an acute incident. The size and shape of the bicipital groove can predispose individuals to instability of the tendon. As mentioned above, the stabilizers of the tendon in the groove are the coracohumeral ligament, the superior glenohumeral ligament, and the subscapularis and supraspinatus tendons. Injury to any or all of these structures can negatively impact the stability of the long head biceps tendon.
LISTEN: ROTATOR CUFF DISCUSSION WITH PREHAB

Treatment for Proximal Biceps Injuries
Conditions that are associated with bicep tendon issues include rotator cuff injuries, subacromial impingement, scapular dyskinesia, lesions of the labrum, and glenohumeral arthritis. Therefore, treatment must address not only the biceps tendon but the surrounding, affected structure(s).
Conservative management for overuse injuries of the biceps tendon must address associated rotator cuff weakness and imbalances across the shoulder girdle and periscapular musculature. Oftentimes, stiff/tight structures, such as pectoralis minor and major, subscapularis, and the posterior glenohumeral joint capsule need to be mobilized, along with mobilization of the thoracic spine to improve the functioning of the shoulder joint complex. Strengthening of the surrounding muscles is also necessary. Additional specific overhead movements must be trained, depending on the individual’s sport or activity.
Want To Learn Some Of The Best Exercises For Biceps Tendinits?
Exercises For Biceps Tendon Pain
Rotator Cuff Strengthening
Sample Biceps Tendon [P]rehab Program Exercise
The rotator cuff muscles are ‘small but loud’! These 4 muscles work together to compress the head of the shoulder within the joint cavity it sits in as we move our shoulder in different planes of movement. If these muscles are not strong or are not working as a team, other components of the shoulder may be predisposed to taking on more load, such as the biceps tendon!

The Prehab membership is the anti-barrier solution to keeping your body healthy. Access state-of-the-art physical therapy, fitness programs, and workouts online in the comforts of your own home or gym! Taking control of your health with exercise & education from the palm of your hand has never been easier. Get access to 50+ programs, 100+ unique workouts, and 3000+ exercises to build your own workout routines. Trial it for free, and learn how to get out of pain, avoid injury, and optimize your health with [P]rehab!
Strengthen The Serratus Anterior!
The serratus anterior plays an integral role in protraction (forward movement) and upward rotation of our shoulder blade. Often times when this muscle is not working properly, the shoulder blade will ‘wing’ and will also lead to compression of structures within the shoulder joint. Want to learn more about how to strengthen the serratus anterior? Read this article!
Posterior Capsule Mobility – Optimize Shoulder Mobility
Sample Biceps Tendon [P]rehab Program Exercise
Glenohumeral internal rotation deficit (GIRD) is a potential cause of biceps tendon pain. This is sometimes due to the back of the shoulder (posterior capsule) being tight. This is a great way to open up the back side of your shoulder!
Don’t Forget The Core!
Remember we must treat the entire person, not just the shoulder! Core weakness is another risk factor for developing biceps tendon pain. The pallof press is a great way to enhance core stiffness, and there are so many awesome variations that can be performed with this movement. Learn more about how to master the pallof press HERE!
Thoracic Spine Mobility
This is one of many great biceps tendon pain exercises. Thoracic spine mobility plays an integral role in shoulder health. Get in a habit of moving your mid back with exercises frequently! If you want to learn more thoracic spine exercises, check out our [P]rehab Thoracic Spine Mobility Overhaul Program!
Other Treatment Options For Biceps Tendon Pain
Corticosteroid injections, such as cortisone can be utilized in conjunction with physical therapy to reduce pain and inflammation around the biceps tendon. As previously stated, corticosteroids can actually increase the risk of tendon rupture so oftentimes, these injections are not placed directly into the tendon itself. Common injection sites are the subacromial space, intra-articular space, bicipital groove, and outside the tendon sheath. A 2011 study documented the accuracy of injections using ultrasound-guided versus blind injections and found that ultrasound-guided injections were done with 87% accuracy whereas the blind injection had an accuracy of just 27%(2).
Want to learn more about cortisone injections? Listen to our [P]Rehab Audio Experience with Dr. Alex Weber!
Surgical Treatment
Bicep tendon tears do not always require surgical intervention as the short head of the biceps tendon can allow for the functioning of the muscle. Treatment would be similar to the conservative measures described above, however surgical intervention may be necessary if conservative treatment fails. Below are a few different approaches to managing biceps tendon pain surgically.
- Biceps tenodesis is an option for partial or full-thickness biceps tendon tears, as well as for biceps tendinopathy, or biceps instability. During this procedure, the long head biceps tendon is detached from its proximal attachment point at the labrum and is then reattached further down the arm at the humerus.
- Biceps tenotomy is similar to the tenodesis procedure with the exception that the tendon is not reattached after being cut. The resultant tendon is left unanchored and retracts down the arm. There is debate about whether tenodesis or tenotomy is the preferred method of surgical intervention for proximal biceps pathologies. Studies show that both procedures are effective at pain reduction, and patients have similar function and strength outcomes. Complication rates are slightly higher with tenodesis procedures. However, tenodesis reduces the risk of developing a Popeye’s sign. Patients undergoing tenotomy have also reported a greater frequency of biceps cramping under heavy loads. With that being said, research does show that patient-reported downsides were often minimal and infrequent in nature and did not alter overall patient satisfaction.(3) Another study reported that both tenotomy and tenodesis patients reported high satisfaction rates at two years post-operative, with 96% of tenodesis patients reporting being satisfied or very satisfied compared to 91% of individuals who underwent tenotomy(4)
- Debridement: Surgical debridement of the biceps tendon is often performed in conjunction with rotator cuff tear repairs or SLAP tear repairs. Surgeons will often choose debridement, which involves smoothing or trimming frayed pieces of the partially torn biceps tendon because it is a relatively simple, safe, and quick adjunct to the rotator cuff or labral repair. This procedure is advantageous as it preserves the structure and anatomy of the biceps tendon.
-
SLAP tears: Surgical options for addressing labral tears include repair of the labrum, debridement of the torn aspects of the labrum, or biceps tenotomy or tenodesis of the long head of the biceps tendon. Labral repairs involve reattaching the torn labrum back to its original location at the top of the shoulder socket. Depending on biceps involvement and presentation, tenotomy or tenodesis may be indicated for the biceps long head tendon. For younger patients with SLAP tears and biceps tendon detachment, anchoring the tendon back to its original place at the supraglenoid tubercle is recommended. Whereas with older adults, a biceps tenodesis or tenotomy is often recommended as blood flow to the labrum is reduced with increasing age and can negatively impact healing and outcomes. There is no definitive agreement on the best surgical management of SLAP tears. Results of debridement of the labrum alone have demonstrated inconsistent outcomes, so repair of SLAP tears is currently the standard (5). A systematic review of SLAP repair outcomes reported 40-94% success rates and 20-94% return to sport, with overhead or throwing athletes having the lowest success rates and return to sport rates (6). Outside of throwing and overhead sport athletes, the study reported overall excellent results for individuals following arthroscopic SLAP repair (6).
Closing Thoughts
Proximal long head biceps tendon pathology is common, but the incidence is low in isolation. For the vast majority, rotator cuff and labrum lesions are present as well as scapular and ligamentous instability, and capsular dysfunction. Conservative measures, including a period of activity modification in conjunction with physical therapy, can reduce symptoms and allow for a safe return to activity. For those who do not respond well to conservative treatment, surgical intervention may be indicated. Prevention is the key to minimizing your risk for a shoulder injury. Check out our Shoulder Prehab Program to start improving your shoulder health today!
Take Ownership of Your Shoulder Health!

To win an NBA championship in this current era it seems at least 3 superstars are needed on the team. Behind these 3 superstars includes the entire support staff that takes care of the day-to-day operations allowing the stars to perform. Sounds like they are using the model of the shoulder! You will learn how to create balance among the support staff which will allow the 3 joints of the shoulder to perform to their superstar abilities!
References
- Abate M, Vanni D, Pantalone A, Salini V. Cigarette smoking and musculoskeletal disorders. Muscles Ligaments Tendons J. 2013;3(2):63-69. Published 2013 Jul 9. doi:10.11138/mltj/2013.3.2.063
- Hashiuchi T, Sakurai G, Morimoto M, Komei T, Takakura Y, Tanaka Y. Accuracy of the biceps tendon sheath injection: ultrasound-guided or unguided injection? A randomized controlled trial. J Shoulder Elbow Surg. 2011;20(7):1069-1073. doi:10.1016/j.jse.2011.04.004
- Meeks BD, Meeks NM, Froehle AW, Wareing E, Bonner KF. Patient Satisfaction After Biceps Tenotomy. Orthop J Sports Med. 2017;5(5):2325967117707737. Published 2017 May 25. doi:10.1177/2325967117707737
- Aflatooni JO, Meeks BD, Froehle AW, Bonner KF. Biceps tenotomy versus tenodesis: patient-reported outcomes and satisfaction. J Orthop Surg Res. 2020;15(1):56. Published 2020 Feb 18. doi:10.1186/s13018-020-1581-3
- Khazai RS, Lee CS, Boyajian HH, Shi LL, Athiviraham A. Rates of Subsequent Shoulder Surgery Within Three Years for Patients Undergoing SLAP Repair Versus Biceps Tenodesis. Arthroscopy, Sports Medicine, and Rehabilitation. 2020;2(2):129-135. doi:ttps://doi.org/10.1016/j.asmr.2020.01.003
- Gorantla K, Gill C, Wright RW. The Outcome of Type II SLAP Repair: A Systematic Review. Arthroscopy: The Journal of Arthroscopic and Related Surgery. 2010;26(4):537-545.
Disclaimer – The content here is designed for information & education purposes only and is not intended for medical advice.
About the author : [P]rehab
Related posts



Latest Blogs

Get Proactive with Prehab
- ✔ Zero wait times, no hidden fees, no barriers to entry!
- ✔ Get out of pain, get stronger, and improve your mobility
- ✔ Access to easy-to-digest physical therapy education videos & resources to learn about your body in the palm of your hand
- ✔ Guidance from trusted Doctors of Physical Therapy








