

Your right kneecap bothers you when you run. It’s not terrible but it just feels different than the left side. It also makes more sounds than the other side when you are squatting or getting up from the couch. Most days, it isn’t a big deal but sometimes it even bothers you going downstairs. You finally go in and see the doctor and they explain that you have “Chondromalacia Patellae” which means the protective cartilage on the back of your kneecap is breaking down. You are now worried that your knee is “bone on bone” and stop doing things that are giving you pain.
In spite of all this, after a few months your knee hurts more than it ever did when you were active. You are doing less and somehow it’s getting worse? Something must be off with this approach. This article will dive into what Chondromalacia Patellae (CMP) is, what it is not, and how you can overcome it.
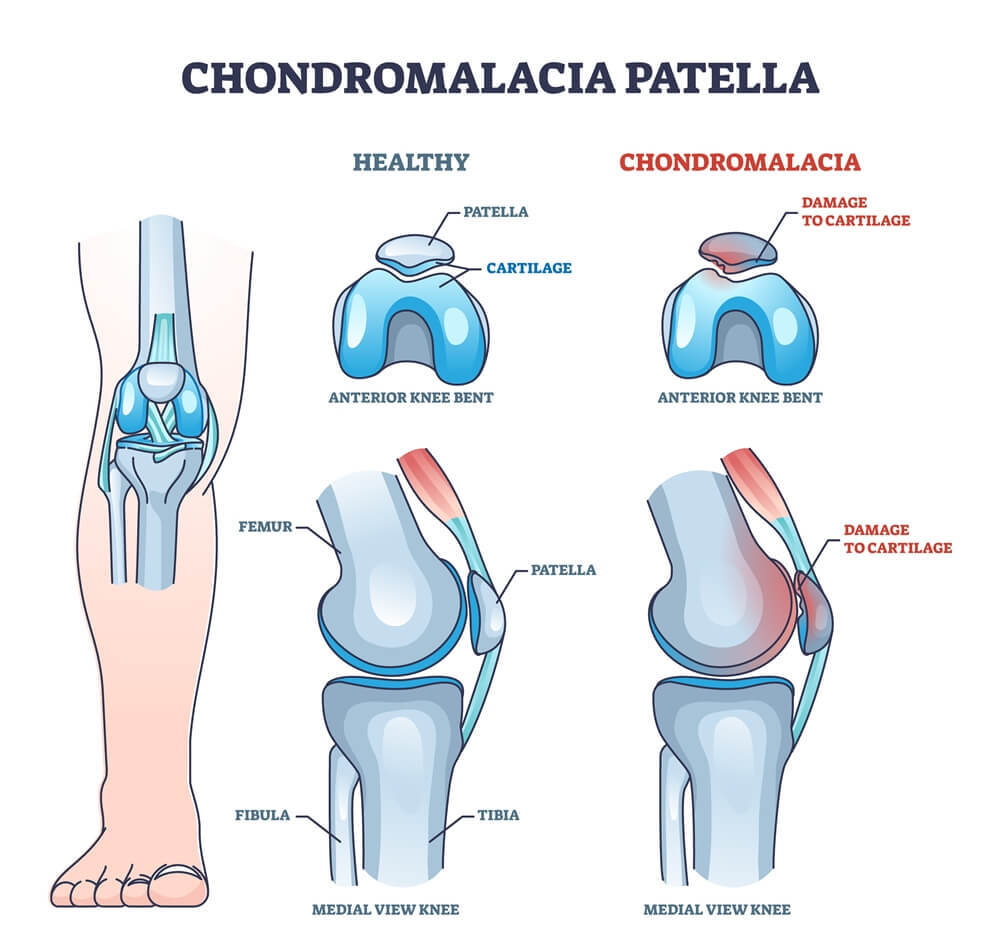
What is Chondromalacia Patellae?
CMP is a description of pain in the front of the knee which translates to “softening of the cartilage.” This refers to the smooth hyaline cartilage on the back of your kneecap which protects the underlying bone. When that cartilage has completely worn away, and there is nothing separating the bones from each other, the condition is called osteoarthritis.
In the case of CMP that level of “bone on bone” has not yet developed and we are instead talking about a decrease in the cushion between your bones. The description of the stages of CMP range from Stage 1-4 with Stage 3 & 4 describing exposure to the bone below the cartilage. This essentially means that stage 3 & 4 CMP are osteoarthritis. This is important to understand as it means that almost nobody who receives a diagnosis of CMP from a doctor has stage 3 or 4 CMP, as they would be told they have osteoarthritis.
LEARN MORE ABOUT OUR PATELLOFEMORAL REHAB PROGRAM

Ready to tackle that knee discomfort once and for all? Get started with our Patellofemoral Rehab program through the app! Designed to get you feeling confident with both decreasing your pain and improving your muscle strength this is the program for you! Get started with a free 7-day trial!
Thus when we are talking about diagnoses of CMP, we are talking about a “thinning” of the cartilage but not cartilage that has been completely worn away exposing bone.
So is thin cartilage causing my knee pain?
Cartilage is aneural meaning it does not have nerve endings and thus cannot be a true source of pain. Thus the logic of CMP as a pain generator rests on two theories:
- Thinning cartilage decreases the cushion between the bones thus potentially generating pain at the bone
- That CMP represents excessive wearing away of that area due to overuse or abnormal biomechanics (typically described as patella maltracking)
These are extremely dubious claims when we consider that even when it comes to knee osteoarthritis (i.e. the most advanced forms of CMP) only as little as 10-20% of people actually have knee pain (1).
READ: THE BEST EXERCISES FOR KNEE OSTEOARTHRITIS

On top of that: up to 43% of asymptomatic individuals over the age of 40 years old showed signs of osteoarthritis on MRI scans (1). This means that nearly half of the people walking around WITHOUT knee pain have signs of the dreaded “bone on bone” diagnosis.

]These statistics alone should call into question the logic of attributing knee pain to “thinning cartilage” but one could argue that OA is more typically diagnosed in middle-aged and older individuals where as CMP is a young person’s diagnosis.
How do We Diagnose CMP?
The typical age range for diagnoses of CMP is 15-35 years old. This diagnosis is usually given based on a clinical exam, meaning your doctor looks at the way you present in their office and gives you a diagnosis of CMP. While X-rays will show osteoarthritis and advanced CMP, they are unable to detect the subtle changes in cartilage volume described in stage 1 and 2 CMP. For this reason, clinical exam is typically the driver of this diagnosis.
The most common test used to diagnosis CMP is called the “Clarke’s Test” or “Patella Grind test” in which the examiner presses down on the patella while asking the patient to contract their quad with reports of pain considered as a positive finding indicative of CMP.
This sounds all well & good, only one problem. A study comparing the Clarke’s test to actual CMP shown via arthroscope determined that “a clinician relying on the Clarke’s Test for the correct diagnosis of CMP would be wrong 38.7% of the time (3).”
This means that if you were diagnosed you with CMP & you are walking around thinking that you have a damaged knee that is causing your pain, there’s a roughly 40% chance that you were diagnosed incorrectly.
Now without signing up for arthroscopic surgery, MRI would be considered the gold standard for accurately showing CMP. Thus, a study was set up to investigate this as well. Researchers compared the cartilage on MRI’s of 64 patients diagnosed with patellofemoral pain and 70 pain-free controls and found that “there is no difference in composition of the patellofemoral cartilage, estimated with multiple quantitative MRI techniques, between patients with PFP and healthy control subjects (4).”
Taken together, these studies tell us that the diagnosis of CMP as the reason for your knee pain is unlikely to be an accurate one and calls into question whether we should be using the term chondromalacia patellae at all. In fact, a large group of world-renowned doctors, physical therapists, and researchers at the 4th International Patellofemoral Pain Research Retreat pondered that exact same question. Their determination? In their 2016 Patellofemoral pain consensus statement they concluded that the term “Chondromalacia Patellae” should no longer be used with the usage of the more accurate “patellofemoral pain” used in its place as the relationship between abnormal joint structure and pain is imprecise (5).
Exercises for Patellofemoral Pain
I’m dealing with Patellofemoral pain, what can be done? Research shows quite a bit! The Patellofemoral Pain clinical guidelines list strengthening of the quadriceps & lateral hip musculature as a level A (their highest) recommendation. They recommended both closed-chain and open-chain knee strengthening. Check out some of the exercises below that fall into this category!
Learn more about these exercises and more in our Patellar Maltracking blog article! Lots can be done from a conservative standpoint to tackle your knee pain discomfort and we encourage you to look into our programming through our Patellofemoral Rehab and Patellofemoral Prehab programs on the Prehab App!
Closing Thoughts
Words matter & the diagnosis of “chondromalacia patellae” tells you that your knee is damaged & being worn away by your activity. It tells you that your pain is the result of structural abnormalities in your knee and that your fragile knee must be protected. Research has shown this to unequivocally be untrue. As we’ve seen above, the methods used by doctors to diagnose CMP in the clinic have nearly a 40% chance of being wrong & MRI studies have shown that kneecap pain has virtually no association with cartilage composition. Patellofemoral pain is complex with a variety of physical and social emotional factors playing a role. We know that associating pain with structural damage is more likely to increase your pain experience & lead you to avoid activities that will strengthen your knee and hip muscles which has the largest impact on decreasing your pain. Don’t let a diagnosis of CMP hold you back from exercise & activity as there is a lot more research showing that these will decrease your pain.
LEARN MORE ABOUT OUR PATELLOFEMORAL REHAB PROGRAM

References:
- Muraki S, Oka H, Akune T, Mabuchi A, En-yo Y, Yoshida M, et al. Prevalence of radiographic knee osteoarthritis and its association with knee pain in the elderly of Japanese population-based cohorts: The ROAD study. Osteoarthritis Cartilage. 2009;17:1137–4
- Culvenor AG, Øiestad BE, Hart HF, Stefanik JJ, Guermazi A, Crossley KM. Prevalence of knee osteoarthritis features on magnetic resonance imaging in asymptomatic uninjured adults: a systematic review and meta-analysis. Br J Sports Med. 2019;53(20):1268-127
- Doberstein ST, Romeyn RL, Reineke DM. The diagnostic value of the Clarke sign in assessing chondromalacia patella. J Athl Train. 2008;43(2):190-196. doi:10.4085/1062-6050-43.2.190
- van der Heijden RA, Oei EH, Bron EE, et al. No Difference on Quantitative Magnetic Resonance Imaging in Patellofemoral Cartilage Composition Between Patients With Patellofemoral Pain and Healthy Controls. Am J Sports Med. 2016;44(5):1172-1178. doi:10.1177
- Crossley KM, Stefanik JJ, Selfe J, et al. 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 1: Terminology, definitions, clinical examination, natural history, patellofemoral
About the Author
Tommy Mandala
[P]rehab Writer & Content Creator
 Tommy Mandala is a Doctor of Physical Therapy, Board Certified Clinical Specialist in Sports & Orthopedics, and Certified Strength and Conditioning Specialist in New York City. He is the founder of ALL IN ACL, a digital coaching platform dedicated exclusively to helping ACLers return to the life they had before their injury with full confidence in their knee. Prior to that, he worked in the sports clinic at Hospital for Special Surgery, the #1 Orthopedic Hospital in the country. While there, he had the opportunity to hone his skills as an ACL specialist working closely with world-renowned surgeons and evaluating patients from all over the world. He completed his sports residency training at the University of Delaware where he had opportunities to work with many of their Division I sports teams as well as the Philadelphia 76’ers NBA G-league affiliate, the Delaware Blue Coats. He also trained at Champion Sports Medicine in Birmingham, Alabama where he had the opportunity to learn from researchers in the American Sports Medicine Institute. Currently, Tommy works exclusively with ACLers through his digital coaching model. While many of these clients are athletes, Tommy works with ACLers of all different abilities helping them to build the strength they need to overcome this unique injury. One of his favorite aspects of his job is taking active clients who have never been a “gym person” before and showing them the amazing things that happen when they learn to strength train.
Tommy Mandala is a Doctor of Physical Therapy, Board Certified Clinical Specialist in Sports & Orthopedics, and Certified Strength and Conditioning Specialist in New York City. He is the founder of ALL IN ACL, a digital coaching platform dedicated exclusively to helping ACLers return to the life they had before their injury with full confidence in their knee. Prior to that, he worked in the sports clinic at Hospital for Special Surgery, the #1 Orthopedic Hospital in the country. While there, he had the opportunity to hone his skills as an ACL specialist working closely with world-renowned surgeons and evaluating patients from all over the world. He completed his sports residency training at the University of Delaware where he had opportunities to work with many of their Division I sports teams as well as the Philadelphia 76’ers NBA G-league affiliate, the Delaware Blue Coats. He also trained at Champion Sports Medicine in Birmingham, Alabama where he had the opportunity to learn from researchers in the American Sports Medicine Institute. Currently, Tommy works exclusively with ACLers through his digital coaching model. While many of these clients are athletes, Tommy works with ACLers of all different abilities helping them to build the strength they need to overcome this unique injury. One of his favorite aspects of his job is taking active clients who have never been a “gym person” before and showing them the amazing things that happen when they learn to strength train.
Disclaimer – The content here is designed for information & education purposes only and is not intended for medical advice.
About the author : Tommy Mandala PT, DPT, SCS, OCS, CSCS
Related posts



Latest Blogs

Get Proactive with Prehab
- ✔ Zero wait times, no hidden fees, no barriers to entry!
- ✔ Get out of pain, get stronger, and improve your mobility
- ✔ Access to easy-to-digest physical therapy education videos & resources to learn about your body in the palm of your hand
- ✔ Guidance from trusted Doctors of Physical Therapy








