

In the musculoskeletal rehabilitative field, we often label different movement and postural pathologies with far-reaching garbage bag terms. Some examples include the upper or lower crossed syndromes, a “SICK” scapula, glenohumeral internal rotation deficit (GIRD), or the subject of this article, scapular dyskinesia. Now, garbage bag terms don’t necessarily mean that these terms are inherently garbage. They often cast a wide net, capturing many musculoskeletal deficits, and providing a general diagnosis for the patient and clinician to work from together. It’s understandable why we use them: generally the patient appreciates having a name attached to the reason behind their pain. However, depending on the training and opinions of the clinician, these terms often receive criticism from those in the healthcare field. Are movement and postural pathologies legitimate? For example, is scapular dyskinesia a medical diagnosis or simply a descriptive term to capture aberrant scapular mechanics? More importantly, what is scapular dyskinesia and how do we define this? Is it truly possible to quantify scapular dyskinesia? And if it’s truly present, does it actually contribute to shoulder pain — and can we make a positive impact with a detailed physical therapy or rehabilitation program? If interested, read on: we’re going to dive into these questions together here.
A brief gross anatomy review: The humerus and scapula

Illustration showing the bones of the shoulder
The shoulder is a complicated place. Extremely mobile in design, it provides for an impressive range of motion. However, with great reward comes great risk; the shoulder is known for instability-based injuries associated with subluxations or dislocations and subsequent labral, bony, or ligamentous injury. Categorized as a ball and socket joint, visualize the humeral head sitting on the glenoid socket like a golf ball resting on a tee. Compare and contrast this to the ball and socket joint of the hip, which is more like a ball sitting within a soup bowl (less range of motion, much more stable). Anatomy provides the framework for function.
Taking our brief gross anatomy review even deeper, the glenoid socket is just one part (an important part mind you) of your scapula. The scapula, commonly referred to as the shoulder blade, provides a stable base of origin for muscles that contribute to dynamic shoulder stability and production of arm motion. Scapular stability is inherently needed for force production from muscles that arise from the scapula (1). A common metaphor that I’ll use with patients in the clinic involves the comparison of the shoulder to a construction crane. The humerus is the arm of the crane, providing far-reaching function. However, the arm of the crane would quickly topple if it didn’t have a stable base (scapula). This being said, one of the larger, consistent themes of shoulder rehabilitation is focusing on strength of the peri-scapular muscles. Working proximally first provides for a stronger base that the humerus can later operate from.
Without this stability, the shoulder couldn’t provide some of the incredible functions that it’s known for in high-level sports: pitching 90+ mph fastballs, working through the extreme ranges of motion involved with swimming or tolerating the wild demands required to perform the rings in Olympic level gymnastics.
Scapular dyskinesia: What is it?
The scapula is a wild piece of anatomy. It’s essentially a free-floating structure suction-cupped to the thorax through numerous muscular attachments and a small bony bridge to the acromion of the scapula. It’s essentially the interposed linkage between the humerus and the axial skeleton (1). This being said, the scapula can do all sorts of cool party tricks: it can depress, retract, protract, tilt, upwardly rotate, and downwardly rotate. Due to its wide range, it holds an extremely important function in regards to overhead motion. In order for the humerus to raise overhead, an impressive force-coupling has to occur to upwardly rotate the scapula. A force-coupling is a series of muscles functioning in relation to one another in order to produce either stability or coordinated movement.
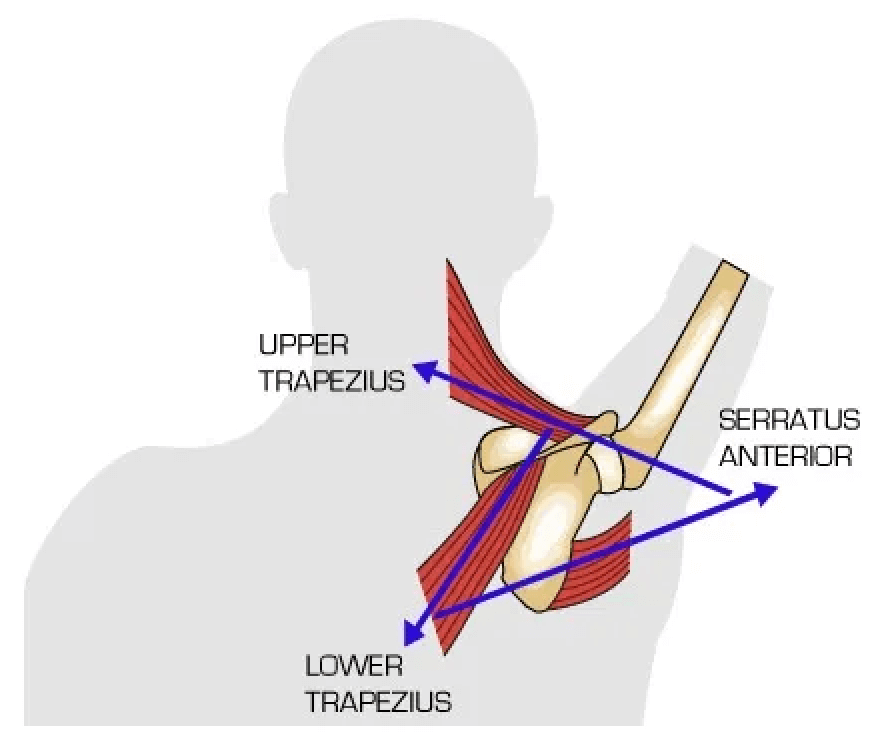
An excellent illustration of scapular upward rotation and the muscular force-coupling the occurs to produce it (2).
For overhead movement to occur, the scapula upwardly rotates through the coordination and strength of the supraspinatus, deltoid, upper trapezius, lower trapezius, and serratus anterior. To dive deep into the nuisances of this relationship is beyond the scope of this blog post, but appreciate there’s a lot of work going on behind the scenes when reaching overhead. To see the line of pull and action of each of these muscles, see the picture above. To learn more, read this article.
READ: HOW OUR SHOULDER MUSCLES WORK TOGETHER

Now, in all good stories exists conflict. In good harmony, the scapula is able to move through its range of upward rotation without issue. However, when this muscular balance is disturbed, and scapular motion or position becomes altered, we call this scapular dyskinesia. It’s important for me to be absolutely clear: scapular dyskinesia is not an injury or a musculoskeletal diagnosis by itself. Rather, it is hypothesized to relate to injury/pain or occur secondarily to changes in shoulder muscle activation, humeral position/motion, and various other mechanisms (1).
Improve Your Scapular Control With Exercises Throughout Our Program!

Throughout our 16-week shoulder [P]Rehab program, we have designed specific exercises to enhance your shoulder blade control, as well as promote optimal shoulder mobility, stability, strength, and function. Get started today!
Quantifying scapular dyskinesia
This is where a considerable amount of debate exists between clinicians, especially those who work almost exclusively with the shoulder (physical therapists and athletic trainers attached to collegiate, MLB teams, or other upper extremity dominant sports). Scapular dyskinesia is certainly a thing — it’s obvious to see the differences between normal and abnormal overhead motion. But in healthcare, we like to quantify things and lean toward being as objective as possible. When we observe scapular dyskinesia, the real questions are: How bad is it really? Is there a reliable scoring system for this? Or is it simply just present or not present? And finally, does this influence the rehabilitation program we build for the patient?
Clinical assessment of scapular dyskinesia is inherently challenging due to the three-dimensional nature of scapular movement and soft tissue surrounding the scapula, often obscuring direct measuring of bony positioning (1). A good clinical evaluation of scapular dyskinesia should contain some basic elements including visual observation to determine the presence or absence of scapular dyskinesis and evaluation of the surrounding anatomic structures that may be responsible for the scapular dyskinesis (we’ll talk about some of these below).
There are several objective scapular dyskinesia grading scales, many of which have been shown to possess adequate levels of reliability (the degree to which the test results can be depended on to be accurate), but the validity (does it measure what it’s actually intended to measure) of most remain questionable due to a lack of direct correlation between scapular dyskinesia and pain. An orthopedic surgeon, Dr. Ben Kibler, is thought to have created the first visually based grading system for scapular dysfunction. He initially defined 3 different types of abnormal scapular motion and 1 normal type in a publication in the Journal of Shoulder and Elbow Surgery (4). Although incredibly well-intentioned and very detailed, this testing scale wasn’t found reliable enough to be utilized in a clinical setting (5, 6).
Kibler’s first scapular dyskinesia scoring system published in the Journal of Shoulder and Elbow Surgery (4). Detailed and well-intentioned, the more complicated the scoring system for scapular dyskinesia, generally the lower reliability.
His grading scale was refined through two more studies and diluted down to a much easier test named the Scapular Dyskinesis Test (SDT) (5). The SDT involves a patient performing weighted shoulder flexion while the clinician visually observes for scapular dyskinesia. In a subsequent study, each shoulder of each subject would get a score of either “normal,” “subtle,” or “obvious.” Much more simple right? Scapular dyskinesia in this study was defined as the presence of either winging (prominence of any portion of the medial border or inferior angle away from the thorax) or dysrhythmia (premature, or excessive, or stuttering motion during elevation and lowering).

Kibler’s initial grading scale was further refined into something much simpler (5). And with this simplification, came greater reliability.
This test held up much better when measured statistically. It had good inter-rater reliability (75% to 82%) and a moderately weighted kappa (0.48 to 0.61), meaning two clinicians could generally find and agree on the same score in a patient. Interestingly enough, however, those with scapular dyskinesia were no more likely to report symptoms (7). This relates back to our note on validity earlier. What’s the point of performing these complicated assessments if they don’t actually correlate to symptoms? Another researcher, Tim Uhl, developed a similar dynamic test for observing scapular dyskinesia (6). He used an even simpler scale of “yes” or “no.” The discussion point here is that Uhl actually looked at a symptomatic group and an asymptomatic group in a subsequent study. The overall prevalence of scapular dyskinesia was essentially equal between those with and without shoulder pain.
This was additionally confirmed in a 2012 systematic review on the diagnostic accuracy of scapular physical examination tests (8). This review found that the presence of scapular dyskinesis or abnormal scapular position is not able to diagnose the presence or absence of shoulder pain (1,8). Furthermore, scapular asymmetries have generally been found to be a common finding in healthy individuals (1,6,9,10). Based on the evidence to date, scapular dyskinesia tests aren’t helpful tests to completely diagnose shoulder pain (1). But surely scapular dyskinesia, when present, means something in the larger picture? But what is it?
Learn How The Serratus Anterior Plays A Key Role In Scapular Stability
I’ve been told I have scapular dyskinesia: Should I care?
In short, probably. However, the way you frame your perception of your scapular dyskinesia is where I caution you to be thoughtful. Many are told by a physician, physical therapist, chiropractor or athlete trainer about how “terribly their scapula moves.” Many are then prescribed weekly physical therapy appointments or a long-term home exercise program to address these deficits, only later told by the same provider about “how much better their scapula moves” when the program is completed. Funny enough, rarely are observable changes in scapular motion, position, or dyskinesia made with our exercise programming (11-13). Yes, you will see providers post on Instagram the before and after videos of scapular mechanics with overhead arm motion. Yes, you can effectively cue patients to make these mechanics improve transiently. But by the time that patient puts their shirt back on, gets in their car to drive home, opens up their cabinet, and grabs a box of cereal from the top shelf subconsciously, I can promise you some level of their dyskinesia has returned.
Now, to effectively dilute my cynicism, please know that peri-scapular strengthening and programming for scapular dyskinesia works. However, while its effect on resolving visual abnormal scapular mechanics is largely debatable, it is consistently demonstrated in the literature that scapular exercises result in higher patient-rated outcomes (14,15). Even in the presence of diagnosed pathology like full-thickness rotator cuff tears or labral tears, exercise programming that included peri-scapular exercise helped a significant amount of patients avoid surgery (up to 80% for full-thickness rotator cuff tears, up to 50% for labral years) (16-19). But to remain realistic – very rarely is a shoulder rehabilitation program exclusively made up of isolated peri-scapular programming. It’s usually included as a subset of exercises within a larger shoulder or arm-care program.
Scapular dyskinesia can be an intimidating phrase to many, often becoming a worry for the upper extremity athlete that they may carry throughout the length of their athletic career. Granted, the by-product of being scared of scapular dyskinesia is often lots of arm-care and careful monitoring of scapular mechanics with overhead movement — and I’m all about arm-care. However, I argue, if we’ve established that scapular dyskinesia alone doesn’t explain shoulder pain and that it’s a relatively common finding in the general public, should we be shaming patients and athletes for their dyskinesia?
LISTEN: How To Manage Shoulder Instability

How do I fix it?
First, lean into the idea that “fixing” your scapular dyskinesia doesn’t mean that it will necessarily look better upon visual inspection. A physical therapist with a well-trained eye will still likely be able to pick apart your aberrant movement patterns as you reach overhead, despite the 8-week arm-care program you completed. However, if you’re struggling with shoulder pain and concurrent findings of scapular dyskinesia — this is where some programming will truly help (symptom-driven results, not aesthetic-driven results). Appreciate that there isn’t a linear or textbook path of how to accomplish this, rather, a good rehabilitative specialist with a strong background in shoulder rehab will likely have their own approach.
Looking at this from a bird’s eye view, there are some basic principles that may be included within your individualized peri-scapular / arm-care programming (20). Not all of these may necessarily be included, but these are some larger themes of what your clinician may prescribe:
Serratus anterior strengthening or retraining: A major muscle in the force-coupling involved with upward rotation of the scapula, strong and healthy serratus is a major theme in the rehabilitation of shoulder pain/scapular dyskinesia. It has a large moment arm for producing scapular motion (21,22,23), and when activation of this muscle is reduced the likelihood of shoulder pain and impingement-related symptoms increases (24,25).
Supine Serratus Scoop-Band
Upper trapezius activation reduction: A “tight” or “over-active” upper trapezius can likely influence excessive clavicular elevation or excessive elevation of the superior border of the scapula.
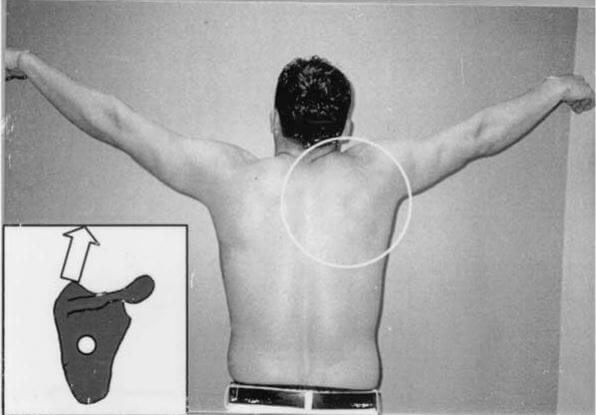
A great photo from some of Kibler’s work (4) demonstrating some aberrant scapular mechanics likely influenced by the upper trapezius.
Prone Scapula Squeeze To Reduce Upper Trap Activation
Posterior shoulder stretching: If tight, the posterior shoulder can alter scapular positioning and influence overhead mechanics. A tight posterior shoulder may pull the scapula into anterior tilt and protraction (26).
Posterior Shoulder Stretch
Pectoralis minor stretching: If tight, the posterior shoulder can alter scapular positioning and influence overhead mechanics, specifically by pulling the scapula into an anterior tilt and internal rotation (20).
Standing Pec Minor Stretch
Thoracic extension posture and exercise: A poor or forward flexed posture can influence how the scapula moves while trying to reach overhead. This is sometimes a surprisingly high-yield intervention in the teenage baseball crowd. Just appreciate that normal thoracic extension is only 10 degrees or less during arm elevation (27), meaning that addressing this alone in isolation, and ignoring the other tips mentioned above, probably won’t offer much. As with most things, it should be included in a comprehensive arm-care program.
Thoracic Spine Extension Mobilization – Foam Roller
Some other general rehabilitative themes should likely be included within a reasonable program (1). Low-load / low-activation exercises with the arm below shoulder level will likely be first (depending on the severity of shoulder pain), allowing for some basic exercises while minimizing the opportunity for any impingement (28). Progression could lead to side-lying and prone exercises that increase load but still allow for the clinician to prescribe exercises focused on lower-trapezius and serratus anterior activation (29). Finally, as tolerance improvements and the effects of progressive loading are noted, later stages of rehabilitation can occur through weight training emphasizing proper retraction and further stabilization principles (30).
Again, a good clinician will be able to guide you through your own personal order of events. Many ways to get to the end goal here.

The Prehab membership is the anti-barrier solution to keeping your body healthy. Access state-of-the-art physical therapy, fitness programs, and workouts online in the comforts of your own home or gym! Taking control of your health with exercise & education from the palm of your hand has never been easier. Get access to 50+ programs, 100+ unique workouts, and 3000+ exercises to build your own workout routines. Trial it for free, and learn how to get out of pain, avoid injury, and optimize your health with [P]rehab!
A note: Medical diagnoses versus movement-impairment syndromes
Much of this article thus far has challenged the idea of scapular dyskinesia as a movement-impairment syndrome. Movement-impairment syndromes are most commonly used by physical therapists to describe various movement aliments — and are often misused or miscategorized, as diagnoses. While well-intentioned, and often wonderfully descriptive in nature, these are not meant to replace medical diagnoses. That being said, while being able to identify scapular dyskinesia as present or non-present is important, there are other important diagnoses that should not be missed based on observation of the scapula and the surrounding musculature. The following medical diagnoses are why clinicians should perform a shoulder examination with the patient’s shirt off. By no means is this list exhaustive.
Long-Thoracic Nerve Palsy: A uncommon condition that can occur from a number of etiologies, most cases are traditionally attributed to an injury or lesion of the long thoracic nerve (31). It usually produces a pretty wild winging of the scapula. The long thoracic nerve innervates the serratus anterior, which helps keep the medial border of the shoulder blade “suction-cupped,” or pulled, flush to the thorax. Denervation, or injury, results in the picture below.

Long thoracic nerve palsy (31).
Suprascapular Cyst: A suprascapular cyst is another somewhat uncommon, but impressive, shoulder pathology. This occurs when a cyst develops over the posterior shoulder, compressing the suprascapular notch. A nerve runs through this notch, the suprascapular nerve, which innervates the supraspinatus and infraspinatus. Upon observation, muscle wasting can occur, alerting a clinician that an orthopedic surgery consultation for possible decompression would be warranted.

An example of supraspinatus and infraspinatus wasting (32). These visual observations can cue in a clinician to more than just scapular dyskinesia.
Spinoglenoid Cyst: Similar to the suprascapular cyst, a spinoglenoid cyst develops a bit lower at the spinoglenoid notch. In this case, wasting would just occur at the infraspinatus, which would alert the observing clinician all the same.
Closing Thoughts
- Scapular dyskinesia is a common finding in abnormal (and normal) shoulders. While it is certainly important to recognize in order to help individualize your rehabilitation programming, it is not the only thing solely responsible for your shoulder pain.
- Exercise programming can help resolve or mitigate your shoulder pain, but will have little influence on resolving how scapular dyskinesia looks with visual observation. Your measure of success should be symptom resolution, not how pleased or displeased the clinician observing the upward rotation of your scapula with overhead movement.
- You can effectively cue those with scapular dyskinesia to look better for a short Instagram or social media video. However, dyskinesia will likely still be present once that patient leaves the clinic, goes about their regular day, and forgets what their clinician was previously instructing.
- A trained clinician will be able to describe the various components of scapular dyskinesia with numerous and complicated descriptors. To be honest, it’s a really impressive skill that takes a keen eye. However, the best way to quantify scapular dyskinesia is likely “normal,” “subtle,” or “abnormal.” Or better yet, “present” or “not present.” Take note, and move on.
- Performing a shoulder exam, especially looking at the upward rotation of the scapula with the shirt off, is important. Yes, it provides insights into scapular dyskinesia, but it can capture other medical diagnoses as well.
- No one is arguing about the benefits of arm care, periscapular strengthening, or rotator cuff strengthening. However, knowing what goals are realistic to shoot for (symptom management) and what outcomes are generally unattainable (perfect scapular mechanics) are very important for patient expectations, time management, and psyche considerations.
Improve Your Scapular Control With Exercises Throughout Our Program!

Throughout our 16-week shoulder [P]Rehab program, we have designed specific exercises to enhance your shoulder blade control, as well as promote optimal shoulder mobility, stability, strength, and function. Get started today!
References
1. Kibler BW, Ludewig PM, McClure PW, Michener LA, Bak K, Sciascia AD. Clinical implications of scapular dyskinesis in shoulder injury: The 2013 consensus statement from the ‘scapular summit.” Br J Sport Med. 2013; 47: 877-885.
2. Neumann DA, Camargo PR. Kinesiologic considerations for targeting activation of scapulothoracic muscles, part 1: Serratus anterior. Brazilian Journal of Physical Therapy. 2019; 23(6): 459-466.
3. Kibler WB, Ludewig PM, McClure PW, et al. Scapula summit 2009. Journal of Orthopedic Sports Physical Therapy. 2009; 39: A1-13.
4. Kibler WB, Uhl TL, Maddux JWQ, et al. Qualitative clinical evaluation of scapular dysfunction: a reliability study. Journal of Shoulder and Elbow Surgery. 2002; 11: 550-556.
5. McClure PW, Tate AR, Kareha S, et al. A clinical method for identifying scapular dyskinesis: part 1: reliability. Journal of Athletic Training. 2009; 44: 160-164.
6. Uhl TL, Kibler WB, Gecewich B, et al. Evaluation of clinical assessment methods for scapular dyskinesis. Arthroscopy. 2009; 25: 1240-1248.
7. Tate AR, McClure PW, Kareha S, et al. A clinical method for identifying scapular dyskinesis: part 2: Validity. Journal of Athlete Training. 2009; 44: 165-173.
8. Wright AA, Wassinger CA, Frank M, et al. Diagnostic accuracy of scapular physical examination tests for shoulder disorders: A systematic review. British Journal of Sports Medicine. 2013; 47 (14): 886-892.
9. Oyama S, Myers JB, Wassinger CA, et al. Asymmetric resting scapular posture in healthy overhead athletes. Journal of Athletic Training. 2008; 43: 565-70.
10. Morais NV, Pascoal AG. Scapular positioning assessment: is side-to-side comparison clinically acceptable? Manual Therapy. 2013; 18: 46-56.
11. Roy JS, Moffet H, Herbert LJ, et al. Effect of motor control and strengthening exercises on shoulder function in persons with impingement syndrome: a single-subject study design. Manual Therapy. 2009; 14: 180-188.
12. McClure PW, Bialker J, Neff N, et al. Shoulder function and 3-dimensional kinematics in people with shoulder impingement syndrome before and after a 6-week exercise program. Physical Therapy. 2004; 84: 832-848.
13. Worsley P, Warner M, Mottram S, et al. Motor control retraining exercises for shoulder impingement: Effects on function, muscle activation, and biomechanics in young adults. Journal of Shoulder and Elbow Surgery. 2013; 22: 11-19.
14. Baskurt Z, Baskurt F, Gelecek N, et al. The effectiveness of scapular stabilization exercise in patients with subacromial impingement syndrome. Journal of Musculoskeletal Rehabilitation. 2011; 24: 173-179.
15. Struyf F, Nijs J, Mollekens S, et al. Scapular-focused treatment in patients with shoulder impingement syndrome: A randomized clinical trial. Clinical Rheumatology. 2013; 32: 73-85.
16. Network MOO. Effectiveness of physical therapy in treating atraumatic full thickness rotator cuff tears. A multi-center prospective cohort study. The american shoulder and elbow surgeons open meeting. San Diego, CA, 2011.
17. Edwards SL, Lee JA, Ball JE, et al. Nonoperative treatment of superior labrum anterior posterior tears: improvements in pain, function, and quality of life. American Journal of Sports Medicine. 2010; 38: 1456-1461.
18. Moore SD, Uhl TL, Sciascia AD, et al. Clinical predictive factors for successful outcome of rehabilitation in patients with SLAP tears. The disabled throwing shoulder: Spectrum of pathology. Lexington, KY, 2011.
19. Fedoriw WW, Ramkumar P, Lintner DM. Nonsurgical and surgical treatment of superior labral tears in professional baseball players. American orthopaedic society for sports medicine. Baltimore, MD, 2012.
20. Ludewig PM, Reynolds JF. The associations of scapular kinematics and glenohumeral joint pathologies. Journal of Orthopedic and Sports Physical Therapy. 2009; 39(2): 90-104.
21. Dvir Z, Berme N. The shoulder complex in elevation of the arm: a mechanism approach. Journal of Biomechanics. 1978; 11: 219-225.
22. Fey AJ, Dorn CS, Busch BP, Laux LA, Hassett DR, Ludewig PM. Potential torque capabilities of the trapezius. Journal of Orthopedic and Sports Physical Therapy. 2007: 37: A44-A45.
23. van der Helm FC. Analysis of the kinematic and dynamic behavior of the shoulder mechanism. Journal of Biomechanics. 1994; 27: 527-550.
24. Lin JJ, Hanten WP, Olson SL, et al. Functional activity characteristics of individuals with shoulder dysfunctions. Journal of Electromyography and Kinesiology. 2005; 15: 576-586.
25. Ludewig PM, Cook TM. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Physical Therapy. 2000; 80: 276-291.
26. Kibler WB. The role of the scapula in athletic shoulder function. The American Journal of Sports Medicine. 1998; 26(2): 325-336.
27. van der Helm FC, Pronk GM. Three-dimensional recording and description of motions of the shoulder mechanism. Journal of Biomechanical Engineering. 1995; 117: 27-40.
28. Cools AM, Dewitte V, Lanszweert F, et al. Rehabilitation of scapular muscle balance. American Journal of Sports Medicine. 2007; 35: 1744-1751.
29. Kibler WB, Sciascia AD, Uhl TL, et al. Electromyographic analysis of specific exercises for scapular control in early phases of shoulder rehabilitation. American Journal of Sports Medicine. 2008; 36: 1789-1798.
30. Ellenbecker TS, Cools A. Rehabilitation of shoulder impingement syndrome and rotator cuff injuries: an evidence-based review. British Journal of Sports Medicine. 2010; 44: 319-327.
31. Martin RM, Fish DE. Scapular winging: anatomical review, diagnosis, and treatments. Curr Rev Musculoskelet Med. 2008;1(1): 1-11.
32. Monterio E, Torres J, Gutierres M, Silva S, Pinto R. An unusual cause of shoulder pain and dysfunction of the shoulder girdle: Parsonage-Turner Syndrome-case report. Eur Orthop Traumatol. 2013.
About The Author
Christopher Lefever, PT, DPT, SCS, CSCS, USAW
[P]Rehab Writer & Content Creator
 Originally from Reading, Pennsylvania, Chris graduated with his bachelor’s degree in exercise science and a doctorate of physical therapy from Slippery Rock University. He afterwards completed a sports physical therapy residency at the Memorial Hermann IRONMAN Sports Medicine Institute. He later completed a division 1 sports physical therapy fellowship at Duke University where he worked closely with Duke football, basketball and lacrosse. He returned to Houston afterwards with Memorial Hermann to help develop an emerging division 1 sports physical therapy fellowship. Present day, he practices with the sports medicine team at the United States Olympic and Paralympic Committee in Colorado Springs, CO. Chris is board certified sports clinical specialist (SCS), certified strength and conditioning specialist (CSCS) and certified in dry needling. He has a particular interest in post-operative rehabilitation of the athletic knee, shoulder, hip and elbow.
Originally from Reading, Pennsylvania, Chris graduated with his bachelor’s degree in exercise science and a doctorate of physical therapy from Slippery Rock University. He afterwards completed a sports physical therapy residency at the Memorial Hermann IRONMAN Sports Medicine Institute. He later completed a division 1 sports physical therapy fellowship at Duke University where he worked closely with Duke football, basketball and lacrosse. He returned to Houston afterwards with Memorial Hermann to help develop an emerging division 1 sports physical therapy fellowship. Present day, he practices with the sports medicine team at the United States Olympic and Paralympic Committee in Colorado Springs, CO. Chris is board certified sports clinical specialist (SCS), certified strength and conditioning specialist (CSCS) and certified in dry needling. He has a particular interest in post-operative rehabilitation of the athletic knee, shoulder, hip and elbow.
Disclaimer – The content here is designed for information & education purposes only and is not intended for medical advice.
About the author : Chris Lefever
Related posts



Latest Blogs

Get Proactive with Prehab
- ✔ Zero wait times, no hidden fees, no barriers to entry!
- ✔ Get out of pain, get stronger, and improve your mobility
- ✔ Access to easy-to-digest physical therapy education videos & resources to learn about your body in the palm of your hand
- ✔ Guidance from trusted Doctors of Physical Therapy








