






Personalized blood flow restriction (BFR) training is a training strategy (or an exercise modality) that involves exercising at low intensities (i.e. 20-35% 1-RM) while occluding venous blood flow out of a limb and restricting arterial blood flow into a limb by using a system that is calibrated based off of personalized limb occlusion pressure. This type of training is accomplished by wrapping off the proximal portion of a limb. In the upper extremity, this is done at the level of the deltoid tuberosity, while in the lower extremity this is performed at the level of the greater trochanter of the femur. As healthcare providers, we recommend using an FDA listed system to perform personalized blood flow restriction training as opposed to other methods such as knee wraps and/or voodoo bands. In this article, we will provide an in-depth review of BFR!
Benefits of BFR: Muscle Hypertrophy and Strength
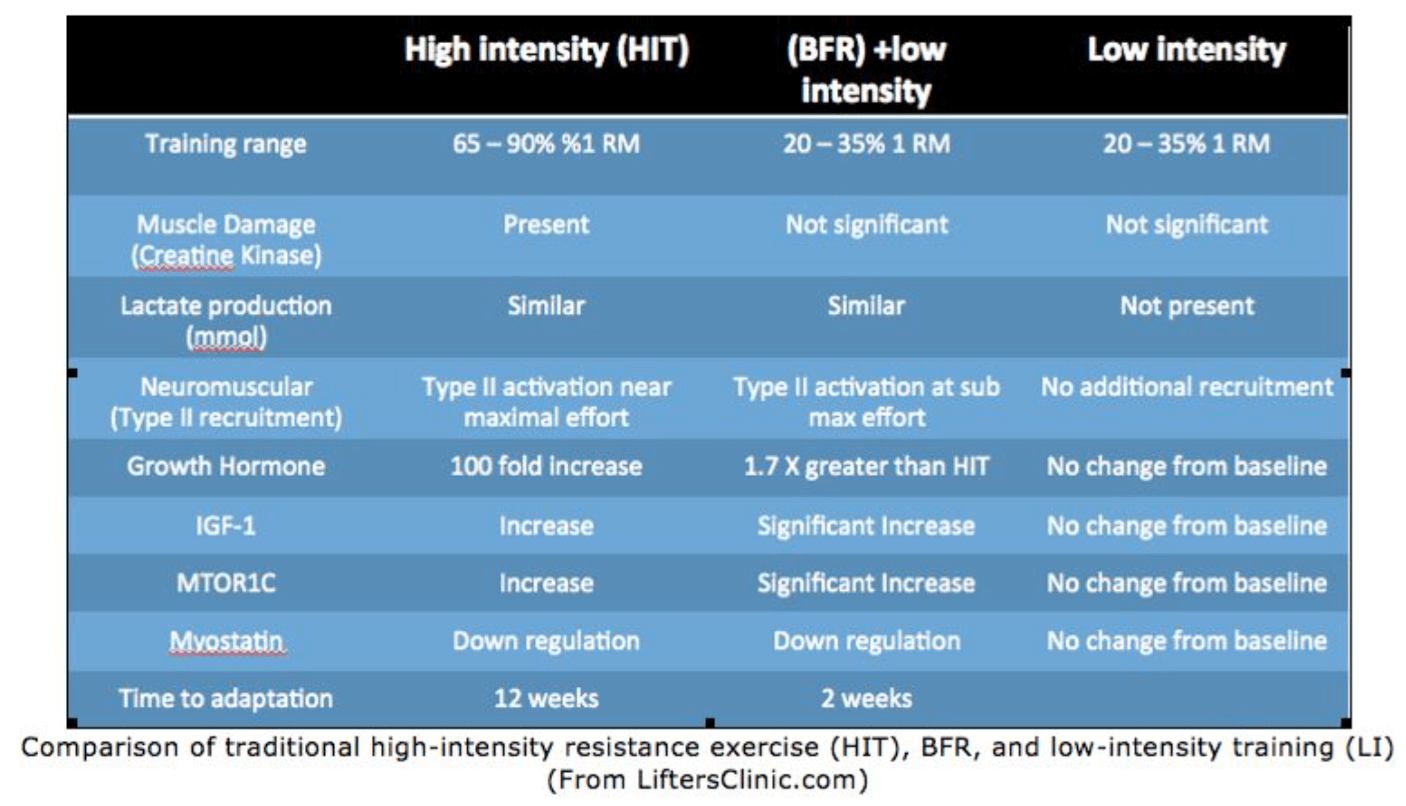
Muscle hypertrophy usually occurs from an overload stimulus produced by progressively increasing an external load using at least 70% of one’s one-repetition maximum (1RM) for a specific lift. This intensity of load is known as HIT or High-Intensity Training. HIT training is defined as using a resistance between 65%-90% of 1RM. For example, if my athlete can max out at 200lbs on a bench press, they would typically need to train with loads of at least 140lbs for 6-8 weeks before hypertrophy would be realized. However, for many individuals, this type of HIT is not possible due to illness or injury. An alternative approach is usually using low resistance like elastic bands to start loading the tissue. Tissue loading low loads can not improve strength or hypertrophy. Most of the benefits of low-load training are neural recruitment. In cases where strength or hypertrophy is needed, Blood Flow Restriction Training (BFRT) can be utilized.
BFRT exercise has been shown to increase muscle hypertrophy and strength at a much lower intensity which may be safer for injured tissue and joints. BFRT combined with low-intensity resistance exercise (20 – 30% 1RM) has been observed to result in significant skeletal hypertrophy and strength within as little as two weeks. In addition, minimal time allowance is necessary to see benefits. Similar to a rehabilitation schedule, low-intensity training combined with BFRT only 2-3 days per week resulted in the greatest effect size compared to training 4-5 days per week. BFRT stimulates muscle hypertrophy by increasing muscle activation and muscle swelling.
A study published in the Journal of strength and conditioning research investigated the acute effects of low-intensity practical BFRT on muscle activation, muscle swelling, and damage. The study concluded that practical BFRT significantly increased muscle activation and muscle thickness without increasing indices of damage to the muscles. Indices of muscle damage are usually found in the blood or urine in the form of creatine kinase. Therefore BFRT enables one to get a high-intensity workout with minimal risk using very lightweight at high repetitions. Compared to standard weight training, BFRT stimulates muscle growth and strength in about half the time and uses about one-third of the weight. By reducing venous return, BFRT forces blood to remain inside your extremities longer than usual. The blood remaining in the muscle leads to faster muscle fatigue and muscle failure, which, in turn, stimulates faster repair and regeneration which results in rapid muscle strength and growth.
Looking for a Program That Will Enhance Your Lower Body Strength?

This program is dedicated to showing love to your lower body, which will make you a more well-rounded individual in regard to exercise or any other activities you love!
Benefits of BFR: Cardiovascular
VO2max is derived from V (volume), O2 (oxygen), and max (maximum). VO2max means the maximum volume of oxygen used during exercise. It is expressed as liters of oxygen per minute (L/minute) or milliliters per kilogram of body weight per minute (mL/kg/minute).
VO2 max is a measure of your cardiorespiratory fitness, especially during prolonged exercise. It is also called maximal oxygen uptake, peak oxygen uptake, maximal oxygen consumption or maximal aerobic capacity.
A study published Journal of Sports Science & Medicine reported that low-intensity (40% VO2 max) cycling exercise short-duration (15 minutes) combined with BFR can produce a significant increase in thigh muscle volume as well as aerobic capacity in young men.[i]
Typically training at about 80% Vo2 for 45 minutes would be required to see this type of enhancement.
What Are the Theories As to Why Personalized Blood Flow Restriction Training Works?
The exact mechanism(s) as to why personalized blood flow restriction works are (are) NOT definitive; however, both mechanical tension AND metabolic stress are thought to be primary driving factors behind hypertrophic and strength adaptations following low-level intensity exercise with personalized blood flow restriction. While it appears that the relationship between metabolic stress and mechanical tension is synergistic in nature, it is thought that metabolic stress is more of a contributing factor. For further explanations, please see the specific sections labeled “Increased Production of Systemic Hormones” as well as “Increased Recruitment of Type II Muscle Fibers.” In addition to the following factors, it is also thought that during low-level exercise with personalized blood flow restriction Myostatin concentrations are decreased, which is a protein responsible for inhibiting muscle hypertrophy but also plays a role in scar tissue formation. In short, whether for prehab, rehab or performance, personalized blood flow restriction is a very effective strategy for adding muscle size and strength while minimizing load to tissues. The problem with saying minimizing breakdown here is when we tie it to performance. One thing we do not want to perpetuate is a belief that personalized blood flow training takes the place of lifting heavy.
READ: WHAT IS INTERNAL LOAD AND LOAD MANAGEMENT?

Mechanical Tension
1. Mechanotransduction
Conversion of mechanical energy into chemical signals that regulate anabolic and catabolic pathways, thus creating a shift that bolsters protein synthesis so that it outweighs protein degradation. For a more detailed understanding of the effects of Mechanotransduction, please see Pearson & Hussain (2015). Reference – Zou et al (2011).
However, the following theorized mechanism is highly questionable, as personalized blood flow restriction is known to result in low mechanical tension. Reference – Pearson & Hussain (2015).
2. Muscle Damage
A systematic review by Loenneke et al (2014) found that overall the literature does NOT support muscle damage as a primary driving force for hypertrophy as seen by….
- NO change in maximum voluntary contraction (MVC). Umbel et al (2009), Loenneke et al (2013a), Thiebaud et al (2013)
- NO increase in blood markers (creatine kinase, lipid peroxide, interleukin-6). Reference – Takarada et al (2000a), Fujita et al (2007), Fry et al (2010)
- NO change in C-reactive protein. Reference – Clark et al (11), Madarame et al (13)
- Muscle soreness ratings are similar to that of submaximal intensities and/or loads. Reference – Umbel et al (2013)
3. Increase Reaction Oxygen Species (ROS) Production
While increased production of ROS has been proposed as a potential mechanism for hypertrophic adaptations following low-level intensity exercise with personalized blood flow restriction, the literature at this point appears conflicting (see Takarada et al 2000 and Goldfarb et al 2008).
Learn How BFR Can Improve Your Training
4. Nitric Oxide (NO)
Since NO production is heavily dependent on high mechanical tension, it would seem that low-level intensity exercise with personalized blood flow restriction would be insufficient to elicit appropriate concentrations of NO to induce hypertrophic adaptations; however, recent studies including Hunt et al (2012, 2013) have demonstrated increased conduit-artery maximal dilation, which is solely dependent on NO production. Thus, the following studies potentially hint at the synergistic nature that metabolic stress plays in conjunction with a mechanical tension. NO has shown to stimulate satellite cell activation and proliferation (Anderson 2000) as well as facilitate mTOR activation, thus directly mediating protein synthesis (Ito et al [2013])
5. Heat Shock Proteins (HSPs)
During times of heat, hypoxia, acidosis, and/or ischemia-reperfusion, HSPs are thought to be elevated to maintain homeostasis. While the evidence is conflicting as to whether or not HSPs contribute to anabolic processes, Pearson & Hussain (2015) hypothesized that maybe certain HSPs (i.e. HSP72 – Kawada & Ishii 2005) and not others (i.e. HSP70 – Fry et al 2010) are elevated during low-intensity exercise + personalized blood flow restriction, thus leading to hypertrophic changes.

The Prehab membership is the anti-barrier solution to keeping your body healthy. Access state-of-the-art physical therapy, fitness programs, and workouts online in the comforts of your own home or gym! Taking control of your health with exercise & education from the palm of your hand has never been easier. Get access to 50+ programs, 100+ unique workouts, and 3000+ exercises to build your own workout routines. Trial it for free, and learn how to get out of pain, avoid injury, and optimize your health with [P]rehab!
Metabolic Stress
1. Increased Production of Systemic Hormones
As opposed to growth hormone (GH) and/or insulin-like growth factor (IGF-1), the better-hypothesized reason appears to be mechano-growth factor (MGH), which may activate a variety of anabolic cascades including mTOR (Sandri 2008), mitogen-activated protein kinase (MAPK) (Barton 2006) and/or calcium-dependent pathways (Tidball 2005) as well as directly resulting in satellite cell activation, proliferation, and differentiation (Yang & Goldspink 2002, Hill et al [2003)
2. Increased Recruitment of Type II Muscle Fibers
Hypoxic environments (i.e. reduced oxygen) AND metabolite accumulation (i.e. blood lactate, Pi, intramuscular pH [via H+ ions]) are hypothesized to result in increased type II muscle fiber recruitment to maintain force production and protect against muscular failure. Reference – Loenneke et al (2011), Yasuda et al (2010
3. Cell Swelling (or Intracellular Hydration)
While previous research has purported that cell-swelling results in increased protein synthesis with a concomitant decrease in proteolysis, such rationalization is highly questionable as the evidence is quite scarce (Pearson & Hussain 2015). For a more detailed explanation as to why cell swelling may result in hypertrophic adaptations, please see the paper by Pearson & Hussain (2015).
4. Muscle Damage (see above)
5. Increased Production Reaction Oxygen Species (ROS) (see above)
LISTEN: [P]REHAB DISCUSSING HOW TO BEGIN STRENGTH TRAINING

Blood Flow Restriction Safety Considerations & Potential Uses
1. Contraindications
For those with a history of deep vein thrombosis (DVTs), hypertension (HTN), varicose veins, and/or cardiovascular disease (CVD) as well as those who are pregnant, personalized blood flow restriction should NOT be used. Reference – Loenneke et al (2011a) & Loenneke et al (2014b).
For further contraindications, please visit this post.
2. Potential Risks
Blood Clots/Thrombus Forming Factors
-
- Personalized blood flow restriction did NOT increase markers of thrombin generation (i.e. prothrombin fragments 1 / 2 OR thrombin-antithrombin III complex [TAT]. Reference – Madarame et al (2010)
Venous Thrombus
-
- When surveying 13,000 people using personalized blood flow restriction (younger than 20 to older than 80), the risk of a venous thrombus was approximately 0.055% (results were confirmed via blood markers including d-dimer, fibrin degradation product, prothrombin time as well a thrombin time. Reference – Nakajima et al (2006)
- After 4 weeks of personalized blood flow restriction training (using 30% 1-RM), neither prothrombin time NOR d-dimer were acutely increased. Reference – Clark et al (2010)
Cerebral Anemia
-
- When surveying 13,000 people using personalized blood flow restriction (younger than 20 to older than 80), the risk of cerebral anemia was approximately 0.277%. Reference – Nakajima et al (2006)
Pulmonary Embolus / Rhabdomyolysis
-
- When surveying 13,000 people using personalized blood flow restriction (younger than 20 to older than 80), the risk for a pulmonary embolism as well as the risk for rhabdomyolysis was approximately 0.008%. Reference – Nakajima et al (2006)
Subcutaneous Hemorrhaging (i.e. bruising)
-
- When surveying 13,000 people using personalized blood flow restriction (younger than 20 to older than 80), the risk for subcutaneous hemorrhaging (or bruising) was approximately 13.1%. Reference – Nakajima et al (2006)
Numbness
-
- When surveying 13,000 people using personalized blood flow restriction (younger than 20 to older than 80), the risk for numbness was approximately 1.297%. Reference – Nakajima et al (2006)
Cold Feeling
-
- When surveying 13,000 people using personalized blood flow restriction (younger than 20 to older than 80), the risk for feeling cold was approximately 0.127%. Reference – Nakajima et al (2006)
Muscle Damage
-
- A systematic review by Loenneke et al (2014) found that overall the literature does NOT support that personalized blood flow restriction with low-intensity exercise can cause increased muscle damage….
- NO prolonged decrease in muscle function
- NO change in maximum voluntary contraction (MVC). Reference – Umbel et al (2009), Loenneke et al (2013a), Thiebaud et al (2013)
- NO change in range of motion (ROM). Reference – Thiebaud et al (2013)
- NO prolonged muscle swelling. Reference – Umbel et al (2009), Wilson et al (2013), Thiebaud et al (2013).
- NO increase in blood markers of muscle damage
- NO change in creatine kinase and/or lipid peroxide. Reference – Takarada et al (2000a)
- NO change in the c-reactive protein. Reference – Clark et al (11), Madarame et al (13)
- Muscle soreness is similar to that of when exercising at submaximal intensities. Reference – Umbel et al (2013)
- NO prolonged decrease in muscle function
- A systematic review by Loenneke et al (2014) found that overall the literature does NOT support that personalized blood flow restriction with low-intensity exercise can cause increased muscle damage….
Peripheral Blood Flow Changes
-
- Similar to exercise without personalized blood flow restriction. Reference – Loenneke et al (2011)
Central Responses of the Cardiovascular System
-
- Blood Pressure
- While the data appears conflicting, Neto et al (2016) highlighted that these changes are within normal limits, thus suggesting that personalized blood flow restriction is a safe alternative to add to an exercise-training program (when cleared by a physician to do so)
- *As highlighted by Dr. Zach Long, blood pressure readings during heavy resistance training have reached as high as 480/350 mmHg as well as 250/190 mmHg just with biceps curls. In comparison, blood pressure readings during low-intensity exercise with personalized blood flow restriction have increased to considerably lower values of 180/100 mmHg.
- Blood Pressure
Blood Pressure
| Low-Intensity Exercise with PBFR vs. Low-Intensity Exercise without PBFR | ||||
| Higher with PBFR | Higher w/o PBFR | No Sig Difference | Higher w/HIT | |
| Takano et al (2005) | ✓ | – | – | – |
| Vieira et al (2013) | ✓ | – | – | – |
| Poton & Polito (2014a) | ✓ | – | – | – |
| Kacin & Strazar (2011) | – | ✓ | – | – |
| Figueroa & Vicil (2011) | – | – | ✓ | – |
| Fahs et al (2012) | – | – | ✓ | – |
| Ozaki et al (2013) | – | – | ✓ | – |
| Low-Intensity Exercise with PBFR vs. Moderate-Intensity Exercise without BPFR | ||||
| Araujo et al (2014) | ✓ | – | – | – |
| Low-Intensity Exercise with & without PBFR vs. High-Intensity Exercise without PBFR | ||||
| Poton & Polito (2014b) | – | – | – | ✓ |
| Poton & Polito (2015) | – | – | – | ✓ |
Interested in joining us for a BFR Course?

Heart Rate
-
- While the data appears conflicting, Neto et al (2016) highlighted that these changes are within normal limits, thus suggesting that personalized blood flow restriction is a safe alternative to add to an exercise-training program (when cleared by a physician to do so).
- *As highlighted by Dr. Zach Long, heart rate readings during heavy resistance training have reached as high as 170 bpm. In comparison, heart rate readings during low intensity exercise with personalized blood flow restriction have increased to considerably lower values of 110 bpm.
Heart Rate
| Low-Intensity Exercise with PBFR vs. Low-Intensity Exercise without PBFR | ||||
| Higher with PBFR | Higher w/o PBFR | No Sig Difference | Higher w/HIT | |
| Takano et al (2005) | ✓ | – | – | – |
| Vieira et al (2013) | ✓ | – | – | – |
| Loenneke et al (2010a) | ✓ | |||
| Poton & Polito (2014a) | ✓ | – | – | – |
| Kacin & Strazar (2011) | – | ✓ | – | – |
| Figueroa & Vicil (2011) | – | – | ✓ | – |
| Fahs et al (2012) | – | – | ✓ | – |
| Loenneke et al (2012) | – | – | ✓ | – |
| Araujo et al (2014) | – | – | ✓ | – |
| Neto et al (2016) | – | – | ✓ | – |
| Low-Intensity Exercise with & without PBFR vs. High-Intensity Exercise without PBFR | ||||
| Poton & Polito (2014b) | – | – | – | ✓ |
| Poton & Polito (2015) | – | – | – | ✓ |
| Fahs et al (2011) | – | – | – | ✓ |
| Rossow et al (2011) | – | – | – | ✓ |
| Brandner et al (2015) | – | – | – | ✓ |
| Okuno et al (2014) | – | – | – | ✓ |
| Hollander et al (2010) | – | – | ✓ | – |
Potential Uses
Prehab To Reduce the Risk of Overuse Lifting Injuries (such as strains and/or tendonitis)
-
- While personalized blood flow restriction has shown to reduce tendon tension (which is beneficial for increasing exercise volume with less risk to soft tissue), it is still hypothesized that we need high intensity resistance training to improve the sufficiency of our tendons to transmit load, which is needed to increase our load tolerance capacity. The reason we say “hypothesized” is because there is research that shows that growth hormone (GH) levels may be elevated up to as much as 290% post-personalized blood flow restriction training. Because we know that GH plays a role in maintaining the ultrastructure of bone, contractile tissue, as well as non-contractile tissue, personalized blood flow restriction, may supply a route of potential tissue resilience similar to that of high-intensity resistance training (Dr. Mario Novo (IG – @liftersclinic).
- Kubo, K., Komuro, T., Ishiguro, N., Tsunoda, N., Sato, Y., Ishii, N., Kanehisa, H., & Fukunaga, T. (2006). Effects of Low-Load Resistance Training with Vascular Occlusion on the Mechanical Properties of Muscle and Tendon. Journal of Applied Biomechanics 22, 112 – 119
- While personalized blood flow restriction has shown to reduce tendon tension (which is beneficial for increasing exercise volume with less risk to soft tissue), it is still hypothesized that we need high intensity resistance training to improve the sufficiency of our tendons to transmit load, which is needed to increase our load tolerance capacity. The reason we say “hypothesized” is because there is research that shows that growth hormone (GH) levels may be elevated up to as much as 290% post-personalized blood flow restriction training. Because we know that GH plays a role in maintaining the ultrastructure of bone, contractile tissue, as well as non-contractile tissue, personalized blood flow restriction, may supply a route of potential tissue resilience similar to that of high-intensity resistance training (Dr. Mario Novo (IG – @liftersclinic).
Rehab
- To Minimize Strength and Hypertrophic Losses Post-Surgically
- Takarada Y, Takazawa H, Ishii N. Applications of vascular occlusion diminish disuse atrophy of knee extensor muscles. Med Sci Sports Exerc, 2000:32 (12); 2035-2039
- To Speed Up the Recovery Process by Loading A Muscle or Joint with Intensities that would Traditionally Require Very High Percentages of One’s 1-RM
- How? Personalized blood flow restriction has been shown to directly influence collagen synthesis, vascular capillary growth, increase signaling of muscle specific stems cells, and alter metabolic function that would otherwise not be seen during the early or sub-acute phases of rehab
- To Treat Acute Injuries (such as muscle strains)
Performance
- To Increase Strength & Hypertrophy when Combined With High Intensity Resistance Training without Decreasing Performance
- Yamanka, T., Farley, R., & Caputo, J. (2012). Occlusion Training Increases Muscular Strength In Division 1A Football Players. Journal of Strength and Conditioning Research 26 (9), 2523 – 2529
- To Maintain Strength & Hypertrophy During Deloading
- O’Halloran, J., Campbell, B., Wilson, J., & Kilpatrick, M. (2014). The Hypertrophic Effects of Practical Vascular Blood Flow Restriction Training.
- To Improve Cardiorespiratory Fitness (i.e. VO2Max)
- Abe, T., Fujita, S., Nakajima, T., Sakamaki, M., Ozaki, H., Ogasawara, R., Sugaya, M., Kudo, M., Kurano, M., Yasuda, T., Ohshima, H., Mukai, C., & Ishii, N. (2010). Effects of Low-Intensity Cycle Training with Restricted Leg Blood Flow on Thigh Muscle Volume and VO2Max In Young Men. J Sports Sci Med 9 (3), 452 – 458.
- To Directly Increase Torque and Power Production
Prehab, Rehab and/or Performance
- To Introduce Intense Exercise without the Fear of Loading (which is especially beneficial for those persons who are unfamiliar with exercise)
General Health Considerations
- To Improve Bone Health, Carotid Arterial Compliance, Vascular Endothelial Function and Peripheral Nerve Circulation (in older adults)
- Hughes, L., Paton B., Rosenblatt, B., Gissane, C., & Patterson, S. (2017). Blood flow restriction training in clinical musculoskeletal rehabilitation: a systematic review and meta-analysis.
BFR Training Frequently Asked Questions
Q: So Why Not Use Knee Wraps or Some Other Device for Personalized Blood Flow Restriction?
Limb occlusion pressure (LOP) is defined as the minimal amount of pressure required to occlude blood flow. When performing personalized blood flow restriction, research has shown that LOP NEEDS to be highly individualized. In other words, personalized blood flow restriction should be performed by taking a certain percentage of one’s LOP, which is based off a variety of factors including limb size, systolic blood pressure, cuff width as well as cuff placement as highlighted by OwensRecoveryScience (IG – @owensrecoverscience). If using knee wraps and/or voodoo bands, this becomes virtually IMPOSSIBLE to account for all these factors and potentially results in higher pressures than what is actually needed. Not only do these unnecessarily higher pressures increase the risk of adverse events (including those that are cardiovascular in nature) but discomfort is increased as well. Additionally, as highlighted by Hughes et al (2017), higher pressures do not translate to greater gains in muscular size, muscular strength, and/or endurance as 40% of one’s LOP has shown similar results to that of 90% of LOP without the increased discomfort. Additionally, devices such as knee wraps and/or voodoo bands are NOT FDA-listed and thus may lead to liability claims if the individual using such methods experiences some sort of injury.
Q: Can I Use Personalized Blood Flow Restriction and Obtain Similar Hypertrophic Changes to that of Heavy Lifting?
You could! While personalized blood flow restriction has shown to stimulate greater hypertrophic changes when compared to low load resistance training without personalized blood flow restriction, it has also shown to result in similar hypertrophic changes to that of high intensity resistance training. (HIRT) However, as mentioned previously, HIRT is still needed to improve the sufficiency of tendons to transmit load, which is needed to increase one’s load tolerance capacity. So if possible, we recommend using both types of training.
Q: Can I Use Personalized Blood Flow Restriction and Obtain Similar Strength Changes to that of Heavy Lifting?
NO! While Personalized Blood Flow Restriction training has shown to stimulate much greater strength changes compared to low load resistance training without personalized blood flow restriction, high intensity resistance training appears to result in greater strength gains compared to personalized blood flow restriction. Interestingly enough, there are some studies using HIRT (i.e. 70% 1-RM) with personalized blood flow restriction which has shown to provide no additional muscle damage compared to HIRT BUT drastically enhances strength gains beyond that of HIRT alone.
Q: Can Personalized Blood Flow Restriction Be Used with Bodyweight Exercises or Does there Need to be an External Load?
Unfortunately, at this point in time, the two studies that have assessed bodyweight exercises vs. external weight directly have found contrary results. If interested, feel free to check out both Kang et al (2015) as well as Head et al (2015), both citations which are listed below. That being said, if we look at a majority of the literature, a lot of the time it has been performed with body weight exercises alone and have shown positive outcomes. Thus, it would appear that external weight is not necessary to stimulate hypertrophic and/or strength adaptations. However, beyond the initial stages of any exercise program, (if appropriate) one should consider adding external load to induce progressive overload.
- Kang, D., Kim, H., Lee, K., & Kim, Y. (2015). The effects of bodyweight-based exercise with blood flow restriction on isokinetic knee muscular function and thigh circumference in college students. International Journal of Physical Therapy Science 27 (9), 2709 – 2712
- Head, P., Austen, B., Browne, D., & Campkin, T. (2015). Effect of practical blood flow restriction training during bodyweight exercise on muscular strength, hypertrophy and function in adults: A randomized controlled trial. International Journal of Therapy and Rehabilitation 22 (6), 263 – 271
Q: Are there Positive Effects on Muscle Groups Proximal to the Cuff?
Lower Extremities – YES
In order to stimulate hypertrophic changes in non – restricted limb musculature in the lower extremity, it appears that resistance training is needed as a study by Sakamaki et al (2011) found that when walking was combined with personalized blood flow restriction that gluteus maximus and lower lumbar (L4-L5) musculature CSA did not change
- Sakamaki, M., Bemben, M., & Abe, T. (2011). Legs and trunk muscle hypertrophy following walk training with restricted leg muscle blood flow. J Sports Sci Med 10, 338 – 340
- Abe, T., Yasuda, T., Midorikawa, T., Sato, Y., Kearns, C., Inoue, K., Koizumi, K., & Ishii, N. (2005). Skeletal muscle size and circulating IGF-1 are increased after two weeks of twice daily “KAATSU” resistance training. International Journal of Kaatsu Training Research 1, 6 – 12
Upper Extremities – YES
- Yasuda, T., Fujita, S., Ogasawara, R., Sato, Y., & Abe, T. (2015). Effects of low-intensity bench press training with restricted arm muscle blood flow on chest muscle hypertrophy: a pilot study. Clinical Physiology and Functional Imaging 30 (5), 338 – 343.
Looking for a Program That Will Enhance Your Lower Body Strength?

How about the character coach Herb Brooks of the USA Men’s Miracle Hockey Olympic team created?!? In training, he once stated, “the legs feed the wolf.” That’s what this program is all about! Landing mechanics from jumping are focused on first along with power via medicine ball slam exercises. If training power, strength is also a must. You dive into our favorite lunge, squat, thrust, and deadlift variations. Lastly, to “fully feed the wolf” cardio and mobility are needed, and don’t worry, it is included!
About the Author
Madison Franek, Physical Therapist
 Madison Franek is a third year doctoral of physical therapy student at Duke University. Prior to beginning graduate school, Madison earned his undergraduate degree in Exercise Science from the University of South Florida where he also became an NSCA certified strength and conditioning coach. While clinically Madison’s interests include injury risk reduction programs (particularly as it relates to the high school athlete), concussion management and blood flow restriction training, he is also passionate about increasing awareness as to the latest scientific research through his Instagram page @evidencebasedmvmt.
Madison Franek is a third year doctoral of physical therapy student at Duke University. Prior to beginning graduate school, Madison earned his undergraduate degree in Exercise Science from the University of South Florida where he also became an NSCA certified strength and conditioning coach. While clinically Madison’s interests include injury risk reduction programs (particularly as it relates to the high school athlete), concussion management and blood flow restriction training, he is also passionate about increasing awareness as to the latest scientific research through his Instagram page @evidencebasedmvmt.
References
- Abe, T., et al. “Skeletal muscle size and circulating IGF-1 are increased after two weeks of twice daily “KAATSU” resistance training.” International Journal of KAATSU Training Research 1.1 (2005): 6-12
- Abe, Takashi, et al. “Effects of low-intensity cycle training with restricted leg blood flow on thigh muscle volume and VO2max in young men.” Journal of sports science & medicine 9.3 (2010): 452.
- Anderson, Judy E. “A role for nitric oxide in muscle repair: nitric oxide–mediated activation of muscle satellite cells.” Molecular biology of the cell11.5 (2000): 1859-1874.
- Clark, B. C., et al. “Relative safety of 4 weeks of blood flow‐restricted resistance exercise in young, healthy adults.” Scandinavian journal of medicine & science in sports 21.5 (2011): 653-662.
- Fry, Christopher S., et al. “Blood flow restriction exercise stimulates mTORC1 signaling and muscle protein synthesis in older men.” Journal of applied physiology 108.5 (2010): 1199-1209.
- Fujita, Satoshi, et al. “Blood flow restriction during low-intensity resistance exercise increases S6K1 phosphorylation and muscle protein synthesis.” Journal of applied physiology 103.3 (2007): 903-910.
- Goldfarb, Allan H., et al. “Resistance exercise effects on blood glutathione status and plasma protein carbonyls: influence of partial vascular occlusion.” European journal of applied physiology 104.5 (2008): 813-819.
- Head, Paul, et al. “Effect of practical blood flow restriction training during bodyweight exercise on muscular strength, hypertrophy and function in adults: A randomised controlled trial.” International Journal of Therapy & Rehabilitation 22.6 (2015).
Hughes, Luke, et al. “Blood flow restriction training in clinical musculoskeletal rehabilitation: a systematic review and meta-analysis.” Br J Sports Med(2017): bjsports-2016. - Hunt, Julie EA, Lucy A. Walton, and Richard A. Ferguson. “Brachial artery modifications to blood flow-restricted handgrip training and detraining.” Journal of applied physiology 112.6 (2012): 956-961.
- Hunt, Julie EA, et al. “Time course of regional vascular adaptations to low load resistance training with blood flow restriction.” Journal of applied physiology 115.3 (2013): 403-411.
- Kang, Dong Yeon, et al. “The effects of bodyweight-based exercise with blood flow restriction on isokinetic knee muscular function and thigh circumference in college students.” Journal of physical therapy science 27.9 (2015): 2709-2712.
- Kawada, S. H. I. G. E. O., and N. A. O. K. A. T. A. Ishii. “Skeletal muscle hypertrophy after chronic restriction of venous blood flow in rats.” Medicine and science in sports and exercise 37.7 (2005): 1144-1150.
- Kubo, Keitaro, et al. “Effects of low-load resistance training with vascular occlusion on the mechanical properties of muscle and tendon.” Journal of applied biomechanics 22.2 (2006): 112-119.
- Loenneke, J. P., et al. “Blood flow restriction: the metabolite/volume threshold theory.” Medical hypotheses 77.5 (2011): 748-752.
- Loenneke, J. P., et al. “Potential safety issues with blood flow restriction training.” Scandinavian journal of medicine & science in sports 21.4 (2011): 510-518.
- Madarame, Haruhiko, et al. “Effects of low‐intensity resistance exercise with blood flow restriction on coagulation system in healthy subjects.” Clinical physiology and functional imaging 30.3 (2010): 210-213.
- Nakajima, T., et al. “Use and safety of KAATSU training: results of a national survey.” International Journal of KAATSU Training Research 2.1 (2006): 5-13.
- Neto, Gabriel R., et al. “Effects of resistance training with blood flow restriction on haemodynamics: a systematic review.” Clinical physiology and functional imaging (2016).
- O’Halloran Jr, John F. The Hypertrophic Effects of Practical Vascular Blood Flow Restriction Training. University of South Florida, 2014.
- Owino, Vivian, Shi Yu Yang, and Geoffrey Goldspink. “Age‐related loss of skeletal muscle function and the inability to express the autocrine form of insulin‐like growth factor‐1 (MGF) in response to mechanical overload.” FEBS letters 505.2 (2001): 259-263.
- Pearson, Stephen John, and Syed Robiul Hussain. “A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy.” Sports medicine 45.2 (2015): 187-200.
- Pope, Zachary K., Jeffrey M. Willardson, and Brad J. Schoenfeld. “Exercise and blood flow restriction.” The Journal of Strength & Conditioning Research27.10 (2013): 2914-2926.
- Sakamaki, Mikako, Michael G. Bemben, and Takashi Abe. “Legs and trunk muscle hypertrophy following walk training with restricted leg muscle blood flow.” Journal of sports science & medicine 10.2 (2011): 338.
- Sandri, Marco. “Signaling in muscle atrophy and hypertrophy.” Physiology23.3 (2008): 160-170.
- Scott, Brendan R., et al. “Exercise with blood flow restriction: an updated evidence-based approach for enhanced muscular development.” Sports medicine 45.3 (2015): 313-325.
- Slysz, Joshua, Jack Stultz, and Jamie F. Burr. “The efficacy of blood flow restricted exercise: A systematic review & meta-analysis.” Journal of Science and Medicine in Sport 19.8 (2016): 669-675.
- Takarada, Yudai, Haruo Takazawa, and Naokata Ishii. “Applications of vascular occlusion diminish disuse atrophy of knee extensor muscles.” Medicine & Science in Sports & Exercise 32.12 (2000): 2035-2039.
- Takarada, Yudai, et al. “Effects of resistance exercise combined with moderate vascular occlusion on muscular function in humans.” Journal of applied physiology 88.6 (2000): 2097-2106.
- Takarada, Yudai, et al. “Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion.” Journal of applied physiology 88.1 (2000): 61-65.
- Thiebaud, Robert S., et al. “Effects of low-intensity concentric and eccentric exercise combined with blood flow restriction on indices of exercise-induced muscle damage.” Interventional Medicine and Applied Science 5.2 (2013): 53-59.
- Tidball, James G. “Mechanical signal transduction in skeletal muscle growth and adaptation.” Journal of Applied Physiology 98.5 (2005): 1900-1908.
- Umbel, Jonathan D., et al. “Delayed-onset muscle soreness induced by low-load blood flow-restricted exercise.” European journal of applied physiology107.6 (2009): 687.
- Yamanaj, Tetsuo, Richard S. Farley and Jennifer L. Caputo. “Occlusion training increases muscular strength in division IA football players.” The Journal of Strength & Conditioning Research 26.9 (2012): 2523 – 2529
- Yasuda, Tomohiro, et al. “Venous blood gas and metabolite response to low-intensity muscle contractions with external limb compression.” Metabolism59.10 (2010): 1510-1519.
- Zou, Kai, et al. “The α 7 β 1-integrin increases muscle hypertrophy following multiple bouts of eccentric exercise.” Journal of Applied Physiology 111.4 (2011): 1134-1141.
Disclaimer – The content here is designed for information & education purposes only and is not intended for medical advice.
About the author : [P]rehab
Related posts




Latest Blogs





